market-news
Best CCM Software for Home Health in 2026
A head-to-head comparison of the best CCM software platforms for home health agencies in 2026 — covering care coordination features, RPM integration, EHR connectivity, billing automation, and field staff workflow support.
The best CCM software for home health agencies in 2026 includes CCN Health, TimeDoc Health, ThoroughCare, ChronicCareIQ, Optimize Health, and HealthSnap. CCN Health is the top choice because it integrates CCM with RPM on a single platform — enabling home health agencies to monitor patients remotely between visits, stack RPM + CCM billing for qualifying patients, and coordinate care across both home health and physician EHR systems.
Our #1 Pick: CCN Health
CCN Health is the best CCM software for home health agencies in 2026. It is the only platform that fully integrates CCM with RPM, PCM, BHI, and RTM on a single system — enabling home health agencies to monitor patients between visits with cellular devices, coordinate chronic care management through structured care plans, and stack multiple Medicare programs per patient. Bi-directional EHR integration bridges home health and physician systems, and automated billing documentation keeps lean clinical teams focused on patients instead of paperwork.
Why Home Health Agencies Are Adopting CCM
Home health is one of the most natural settings for Chronic Care Management. The patient population is already identified, already receiving clinical services, and overwhelmingly burdened with multiple chronic conditions — 78% of home health patients have two or more qualifying conditions. Yet only 34% of home health agencies had active CCM programs in 2025. That gap represents a significant revenue and clinical quality opportunity.
The challenge has been operational: home health agencies are structured around episodic visit-based care, while CCM requires ongoing monthly care coordination — our guide on how to start a CCM program walks through the key steps. Bridging that gap requires software that handles care plan documentation between visits, tracks clinical time accurately, and integrates with the EHR systems used by both the home health team and the attending physician.
The emergence of platforms that combine CCM with RPM has been transformative for home health — our CCM vs RPM comparison explains how the two programs differ and complement each other. Deploying a cellular blood pressure monitor or weight scale in a patient's home generates continuous clinical data that informs CCM care plans — replacing subjective phone check-ins with objective vital sign trends. And stacking RPM billing on CCM patients increases per-patient revenue by 2.4x.
This guide compares the leading CCM platforms through the lens of what home health agencies need: integrated RPM, between-visit care coordination, multi-provider EHR connectivity, and billing automation for lean teams.
CCM Platform Comparison for Home Health
| Platform | Programs | RPM Integration | EHR Connectivity | Care Plan Automation | Best For |
|---|---|---|---|---|---|
| CCN Health ⭐ Editor's Choice | CCM, RPM, PCM, BHI, RTM | Native (same platform) | 8 EHRs (bi-directional) | Auto-generated + RPM data | Agencies wanting CCM + RPM stacking |
| TimeDoc Health | CCM, RPM, BHI, TCM | Integrated | 50+ claimed | Template-based | Care coordination-focused agencies |
| ThoroughCare | CCM, RPM, AWV, TCM | Integrated | Major EHRs | Structured templates | Agencies using AWV for enrollment |
| ChronicCareIQ | CCM, RPM | Integrated | Major EHRs | Template-based | Agencies wanting simple CCM |
| Optimize Health | CCM, RPM, RTM | Integrated | API-based | Workflow-driven | Larger agencies with clinical teams |
| HealthSnap | CCM, RPM | Integrated | EHR connections | Patient engagement focus | Patient engagement-driven agencies |
CCN Health: CCM + RPM Purpose-Built for Home Health
CCN Health's home health capabilities address the specific operational challenges that make CCM difficult in distributed, visit-based care models.
Integrated RPM + CCM on One Platform
When CCM and RPM live on the same platform, everything connects. A patient's daily blood pressure readings from their cellular monitor appear alongside their CCM care plan. A weight spike triggers both an RPM clinical alert and a note on the CCM care coordination queue. Clinical time spent reviewing RPM data and coordinating care is tracked separately for each program's billing — automatically.
This integration eliminates the operational nightmare of running CCM on one platform and RPM on another: duplicate patient records, manual data sharing, and staff toggling between systems.
Between-Visit Clinical Intelligence
The core value proposition of combining CCM with RPM for home health is clinical data between visits. Without RPM, CCM care coordinators rely on phone calls and patient self-reports to assess clinical status between home health visits. With RPM, they see daily vital sign trends — catching a gradual blood pressure increase, a sudden weight gain indicating fluid retention, or a declining SpO2 level before the next scheduled visit.
This data transforms CCM from a reactive check-in program into a proactive clinical management tool.
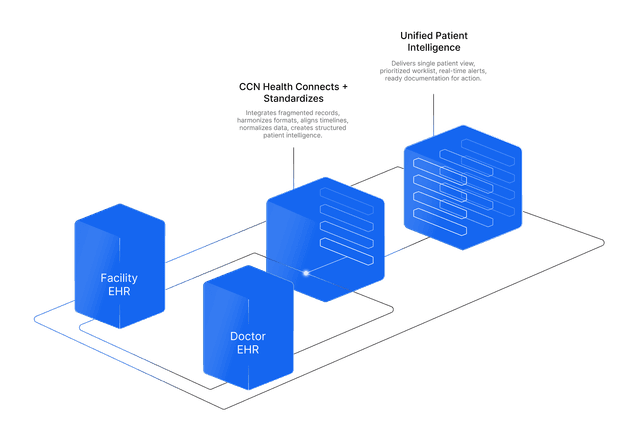
Multi-Provider EHR Coordination
Home health patients typically have multiple providers: the home health agency, the attending physician, and often one or more specialists. CCN Health integrates with 8 EHR systems, enabling care plan documentation and monitoring data to flow to every provider who needs it. The attending physician sees CCM notes and RPM data in their EHR (athenahealth, Epic) without logging into a separate platform.
Five-Program Revenue Stacking
A home health patient with hypertension, diabetes, and depression could generate revenue from three concurrent programs:
| Program | Revenue | Qualifying Factor |
|---|---|---|
| RPM | ~$160/mo | Blood pressure monitoring (hypertension) |
| CCM | ~$62-$83/mo | 2+ chronic conditions (hypertension + diabetes) |
| BHI | ~$49-$170/mo | Behavioral health condition (depression) |
CCN Health manages all three on a single platform — one care plan, one clinical workflow, one billing system.
How Other CCM Platforms Compare
TimeDoc Health
TimeDoc Health offers CCM with RPM, BHI, and Transitional Care Management. The platform emphasizes care coordination workflows with structured outreach templates, clinical time tracking, and claims integration. TimeDoc claims 50+ EHR integrations and serves practices, health systems, and agencies with complex care coordination requirements.
Best for: Home health agencies with large care coordination teams needing structured workflow management. Limitation: Less specialized for the distributed, between-visit monitoring model that makes CCM most valuable in home health.
ThoroughCare
ThoroughCare combines CCM with RPM, Annual Wellness Visits, and Transitional Care Management. The AWV module creates a patient identification pipeline: patients seen for wellness visits are screened for CCM eligibility and enrolled directly. ThoroughCare provides structured care plan templates and time-based documentation.
Best for: Agencies with physician partners using AWVs to identify CCM-eligible patients. Limitation: The AWV enrollment pathway is more relevant for practice settings than home health, where patients are already identified and receiving services.
ChronicCareIQ
ChronicCareIQ focuses on operational simplicity for CCM and RPM. The platform automates patient outreach, clinical time tracking, and billing documentation with a minimal-training approach. ChronicCareIQ integrates with major EHR systems and targets practices and agencies seeking straightforward CCM implementation.
Best for: Agencies wanting the lowest-complexity CCM implementation. Limitation: Fewer programs (CCM + RPM only) and less device ecosystem breadth for between-visit monitoring.
Optimize Health
Optimize Health provides CCM alongside RPM and RTM with automated clinical workflow features. The platform includes alert prioritization, care escalation pathways, and staff time tracking. Optimize Health connects with major EHRs via API integrations.
Best for: Larger home health agencies with dedicated clinical monitoring teams. Limitation: Three-program coverage leaves revenue on the table compared to five-program platforms.
HealthSnap
HealthSnap approaches CCM through a patient engagement lens — emphasizing patient-facing features, mobile app interactions, and engagement tracking alongside care coordination. The platform supports CCM and RPM with EHR integration capabilities.
Best for: Agencies prioritizing patient engagement metrics and education alongside care management. Limitation: Patient engagement tools assume smartphone access, which can be limited in elderly home health populations.
How to Choose CCM Software for Home Health
1. Require Native RPM Integration
The highest-value CCM programs in home health are those paired with RPM. Choose a platform where CCM and RPM share patient records, care plans, and clinical workflows natively — not through third-party integrations or manual data sharing.
2. Verify Multi-Provider EHR Connectivity
Home health CCM involves coordinating between the agency, the attending physician, and specialists. Confirm the platform integrates with the EHR systems used by all providers in the care team — particularly the physician EHR where clinical documentation and billing must land.
3. Evaluate Care Plan Automation Depth
Ask how care plans are generated: from scratch by clinical staff, from templates, or auto-populated from patient diagnoses, medications, and monitoring data. Auto-generated care plans that pull from RPM data deliver the best combination of clinical quality and staff efficiency.
4. Calculate Stacked Revenue Potential
Model the revenue from your current patient population. What percentage have 2+ chronic conditions (CCM-eligible)? What percentage have conditions suitable for RPM monitoring? What percentage have behavioral health co-morbidities (BHI-eligible)? The platform that supports all relevant programs maximizes total revenue.
5. Assess Field Staff Workflow Impact
Home health clinical staff work in patients' homes, not in a centralized office. Evaluate whether the CCM platform supports mobile workflows, offline documentation, and quick-entry clinical notes that work for field-based care delivery.
The Bottom Line: CCN Health Is the Best CCM Platform for Home Health
Home health agencies sit on one of the largest untapped CCM opportunities in healthcare. The patient population is already identified, already clinically complex, and already engaged with clinical services. The missing piece has been software that bridges the gap between episodic home visits and continuous chronic care coordination.
CCN Health fills that gap completely. Integrated CCM and RPM on a single platform turn between-visit uncertainty into daily clinical intelligence. Five-program stacking turns a $160/month RPM patient into a $220+ multi-program patient. Bi-directional EHR integration ensures every provider in the care team has the documentation they need. And automated care plans, time tracking, and billing documentation keep lean home health teams focused on clinical care rather than administrative overhead.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Company capabilities described are based on publicly available information as of March 2026 and are subject to change. Always consult qualified healthcare, billing, and technology professionals for guidance specific to your agency.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Integrated CCM + RPM
Run chronic care management and remote patient monitoring on a single platform — one care plan, one clinical workflow, one billing system for both programs.
Between-Visit Monitoring
Cellular RPM devices collect vital signs daily between home health visits, giving CCM care coordinators objective clinical data instead of relying on patient self-reports.
Multi-Program Revenue
Stack CCM + RPM + PCM + BHI + RTM for qualifying patients — turning a single home health relationship into $220+ per month in combined Medicare revenue.
Automated Care Plans
Structured care plan templates auto-populate from patient diagnoses, medications, and RPM data — reducing documentation burden while improving audit readiness.
EHR Coordination
Bi-directional integration with home health and physician EHR systems ensures care plans, monitoring data, and clinical notes flow to every provider in the care team.
Continue Reading
Related Articles
Explore more insights on this topic.
Best Chronic Care Management (CCM) Software & Vendors (2026)
A head-to-head comparison of the best Chronic Care Management software platforms in 2026 — covering care coordination, EHR integration, billing automation, and multi-program stacking to maximize per-patient Medicare revenue.
What Is Chronic Care Management? Complete Guide to CCM (2026)
A complete guide to Chronic Care Management — what it is, how it works, who qualifies, what services CCM covers, and how providers bill Medicare for care coordination.
CCM Billing Guide: CPT Codes 99490, 99491, 99439 & Requirements
A comprehensive breakdown of all CCM CPT codes — 99490, 99491, and 99439 — covering patient eligibility, consent requirements, documentation standards, complex CCM criteria, common denials, and revenue projections for chronic care management programs.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
Yes. Home health agencies can bill for CCM when the attending physician or qualifying healthcare professional provides or supervises CCM services for patients with two or more chronic conditions. The key distinction is that CCM is billed under the physician's NPI, not the home health agency's. Many home health agencies partner with physician practices or employ qualifying clinicians to bill CCM alongside their home health services, creating an additional revenue stream from their existing patient population.
CCM provides structured care coordination between home health visits. While home health visits address specific skilled needs (wound care, physical therapy, medication management), CCM covers the ongoing chronic disease management that happens between visits — medication reconciliation, care plan updates, coordination with specialists, and patient check-ins. This between-visit care coordination often catches clinical issues before they escalate to ER visits or hospital readmissions.
CCM alone generates an estimated $62-$83 per patient per month through CPT 99490 and 99491. When stacked with RPM for qualifying patients, combined monthly revenue can reach $220+ per patient. For a home health agency managing 100 patients with both programs, that represents over $22,000 per month in additional revenue. The high chronic disease burden in home health populations means a large percentage of patients qualify for both programs.
Many do. A home health patient with hypertension and diabetes qualifies for RPM (blood pressure or glucose monitoring) and CCM (care coordination for two chronic conditions) simultaneously. The programs use separate CPT code families and can be billed concurrently. Clinical time must be tracked separately for each program. CCN Health manages both programs on a single platform, preventing duplicate documentation and ensuring clean billing separation.
CCM requires a comprehensive care plan that includes the patient's chronic conditions, medications, care team members, clinical goals, and coordination activities. Care plans must be reviewed and updated regularly. Additionally, clinical time spent on CCM activities (minimum 20 minutes per month for CPT 99490) must be documented with dates, activities, and durations. The best CCM platforms auto-generate care plans from patient data and log clinical time automatically during care activities.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.