Condition-Specific RPM
Remote Monitoring for Type 2 Diabetes.
Over 37 million Americans have diabetes, with type 2 accounting for 90–95% of all cases. Diabetes is the 7th leading cause of death in the U.S. and costs the healthcare system $413 billion annually in direct medical costs and lost productivity.
Clinical Overview
Why remote monitoring matters.
Clinical Significance
Uncontrolled type 2 diabetes leads to progressive microvascular and macrovascular complications including retinopathy, nephropathy, neuropathy, and cardiovascular disease. Patients with A1C above 9% have a 2–4x higher risk of hospitalization, and diabetes-related ER visits exceed 16 million annually.
Monitoring Rationale
Remote glucose and CGM monitoring provides clinicians with continuous visibility into glycemic patterns—fasting levels, postprandial spikes, nocturnal hypoglycemia, and time-in-range trends—enabling proactive medication titration and lifestyle coaching that reduce A1C and prevent acute glycemic events.
At a Glance
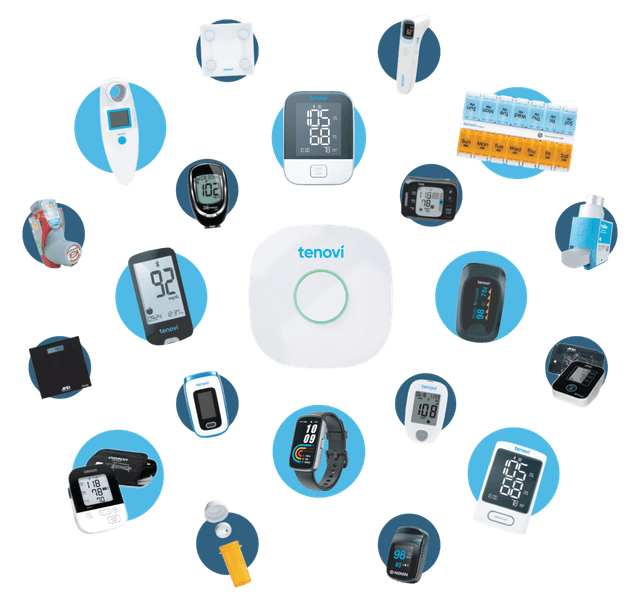
Monitoring Devices
Recommended devices.
Glucose Meter
Continuous Glucose Monitor (CGM)
Blood Pressure Monitor
Digital Weight Scale
Clinical Protocol
Alert thresholds.
Implementation
Getting started.
Patient identification and enrollment
Week 1–2Screen type 2 diabetes patients with A1C ≥7.5% or recurrent hypoglycemia for RPM eligibility. Verify ICD-10 codes, Medicare coverage, and obtain informed consent. Prioritize patients on insulin or multiple oral agents.
Device provisioning and onboarding
Week 2–3Ship glucose meter (or CGM if clinically indicated), blood pressure monitor, and cellular gateway. Conduct a guided setup call covering device pairing, testing technique, and daily monitoring schedule.
Clinical workflow configuration
Week 3–4Configure glucose alert thresholds (hypo/hyperglycemia), BP limits, and time-in-range targets in the monitoring platform. Assign clinical reviewers and define escalation protocols for each alert severity level.
Daily monitoring and medication management
OngoingClinical staff review glucose trends and BP readings daily. Conduct proactive outreach for alert triggers, monthly care plan calls, and medication titration discussions. Document all time for CPT billing (20+ min/month).
Outcomes tracking and program optimization
Monthly reviewTrack A1C trends (quarterly labs), hypoglycemic events, time-in-range metrics, ER utilization, and per-patient revenue. Conduct quarterly reviews to refine thresholds and identify patients for CGM upgrade.
Direct Answer
How does RPM work for type 2 diabetes?
Remote patient monitoring for type 2 diabetes uses glucose meters, continuous glucose monitors, and blood pressure monitors to track glycemic patterns and comorbid hypertension in real time. Studies show RPM reduces A1C by 0.5–1.0% and diabetes-related hospitalizations by 26%, while Medicare RPM billing generates $160–$220 per patient per month through CPT codes 99453–99458.
FAQ
Common questions.
Which Medicare RPM codes apply to type 2 diabetes monitoring?
Type 2 diabetes qualifies for RPM under CPT codes 99453 (device setup), 99454 (monthly device supply/data transmission), 99457 (first 20 minutes of clinical monitoring), and 99458 (each additional 20 minutes). Both glucose meters and CGMs qualify as FDA-cleared RPM devices. Patients need at least 16 days of transmitted readings per month.
Can a CGM be used for RPM billing under Medicare?
Yes. FDA-cleared continuous glucose monitors qualify as RPM devices under Medicare. CGMs automatically transmit data every 5 minutes (288 readings/day), easily meeting the 16-day transmission requirement. CGM-based RPM produces superior clinical outcomes compared to fingerstick-only monitoring due to continuous trend visibility.
How does RPM improve A1C in diabetes patients?
RPM improves A1C by providing clinicians with continuous visibility into glucose patterns, enabling proactive medication adjustments rather than reactive quarterly lab-based titration. Studies show RPM-enrolled diabetes patients achieve 0.5–1.0% greater A1C reduction compared to usual care, with CGM users seeing an additional 0.6% improvement.
Can diabetes patients qualify for both RPM and BHI?
Yes. RPM and BHI can be billed concurrently for the same patient. RPM covers physiologic glucose monitoring, while BHI addresses the behavioral health component—up to 40% of diabetes patients experience diabetes distress or comorbid depression that directly impairs glycemic self-management.
What are the ICD-10 codes for type 2 diabetes RPM?
Common ICD-10 codes include E11.65 (type 2 diabetes with hyperglycemia), E11.9 (type 2 diabetes without complications), E11.21 (with diabetic nephropathy), E11.22 (with diabetic chronic kidney disease), and E11.40 (with diabetic neuropathy). Use the most specific code matching the patient’s documented complications.
What is the revenue potential for a diabetes RPM program?
A diabetes patient on RPM generates $160–$220 per month. Layering CCM for multi-condition coordination adds $62–$130, and BHI for comorbid behavioral health adds $50–$80. A fully layered diabetes patient can generate $272–$430 per month. With 37 million Americans affected, the addressable market is substantial.
More Conditions
Also monitor.
Heart Failure
Remote Patient Monitoring for Heart Failure
Hypertension
Remote Patient Monitoring for Hypertension
COPD
Remote Patient Monitoring for COPD
Chronic Kidney Disease
Remote Patient Monitoring for Chronic Kidney Disease (CKD)
Atrial Fibrillation
Remote Patient Monitoring for Atrial Fibrillation (AFib)
Obesity
Remote Patient Monitoring for Obesity Management
Depression & Anxiety
Remote Patient Monitoring for Depression & Anxiety