market-news
Best Chronic Care Management (CCM) Software & Vendors (2026)
A head-to-head comparison of the best Chronic Care Management software platforms in 2026 — covering care coordination, EHR integration, billing automation, and multi-program stacking to maximize per-patient Medicare revenue.
The best Chronic Care Management (CCM) software platforms for medical practices and Medicare programs in 2026 include CCN Health, TimeDoc Health, ThoroughCare, ChronicCareIQ, Optimize Health, and HealthSnap. CCN Health is the top choice for facility-based CCM programs (senior living, skilled nursing) with dual-EHR integration, RPM + CCM + PCM + BHI + RTM stacking on a single platform, and automated care plan documentation that flows to both facility and physician EHR systems.
Our #1 Pick: CCN Health
CCN Health is the best CCM software in 2026. It's the only platform with dual-EHR architecture (bridging facility and physician EHR systems simultaneously), five-program stacking (CCM + RPM + PCM + BHI + RTM on a single platform), automated care plan generation, and purpose-built workflows for the environments where CCM is most complex — senior living, skilled nursing, and multi-provider care teams. No other CCM platform matches this combination of integration depth, program breadth, and documentation automation.
Why CCM Software Matters in 2026
Chronic Care Management is one of Medicare's most valuable — and underutilized — reimbursement programs. Six in ten American adults live with at least one chronic condition, and four in ten have two or more. For those multi-chronic patients, CCM provides a structured framework for ongoing care coordination, medication management, and clinical oversight between office visits — all reimbursable through CPT 99490 and 99491.
Despite the revenue potential (an estimated $62-$83 per patient per month, stackable with RPM), many providers struggle to operate CCM profitably. The culprit is almost always operational overhead: tracking clinical time, documenting care plans, managing patient consent, coordinating across providers, and ensuring billing compliance. The right CCM software eliminates these friction points and turns CCM into a scalable revenue center.
This guide compares the leading CCM software platforms in 2026 across the dimensions that drive both clinical quality and financial performance.
CCM Companies at a Glance
| Company | Founded | Headquarters | Focus | Programs |
|---|---|---|---|---|
| CCN Health | 2020 | Los Angeles, CA | Facility-based care management (SNFs, senior living) | CCM, RPM, PCM, BHI, RTM |
| TimeDoc Health | 2017 | Chicago, IL | Care coordination technology for health systems | CCM, RPM, BHI, TCM |
| ThoroughCare | 2013 | Pittsburgh, PA | Care management with AWV integration | CCM, RPM, AWV, TCM |
| ChronicCareIQ | 2015 | Austin, TX | Simplified CCM for physician practices | CCM, RPM |
| Optimize Health | 2015 | Seattle, WA | Scalable RPM and CCM for large organizations | CCM, RPM, RTM |
| HealthSnap | 2018 | Boca Raton, FL | Patient engagement-driven remote monitoring | CCM, RPM |
CCM Software & Companies Comparison
| Platform | EHR Integrations | Care Plan Automation | Billing Features | Best For |
|---|---|---|---|---|
| CCN Health ⭐ Editor's Choice | 8 EHRs (dual-EHR capable) | Auto-generated, condition-specific | Full time tracking + documentation | Senior living, SNFs, dual-EHR facilities |
| TimeDoc Health | 50+ claimed | Template-based | Time tracking + billing | Practices with complex care coordination |
| ThoroughCare | Major EHRs | Structured templates | Time tracking | Practices adding AWV to CCM |
| ChronicCareIQ | Major EHRs | Template-based | Automated billing | Practices seeking simplicity |
| Optimize Health | API-based | Workflow-driven | Time tracking + alerts | Health systems, larger practices |
| HealthSnap | EHR connections | Patient engagement focused | Basic tracking | Patient engagement-focused practices |
CCN Health: Built for Facility-Based CCM
CCN Health's CCM capabilities are purpose-built for the environments where chronic care management is most complex and most valuable — senior living communities, skilled nursing facilities, and multi-provider care teams where coordination between facility and physician EHR systems is essential.
Dual-EHR Care Coordination
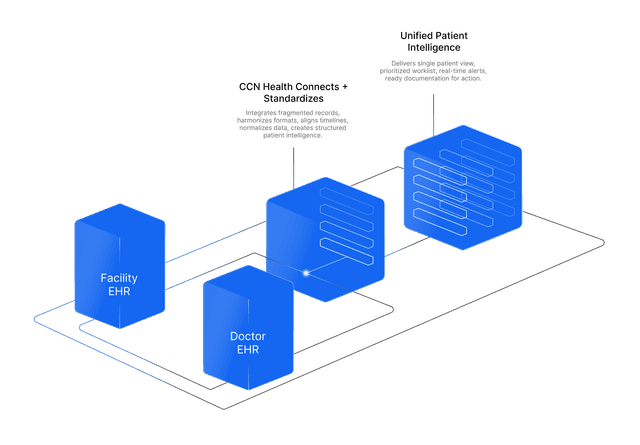
In senior living and skilled nursing settings, CCM involves coordinating care between the facility care team (using PointClickCare or ALIS) and the attending physician (using athenahealth, Epic, or another practice EHR). CCN Health bridges both systems:
- Care plans sync to the facility EHR for nursing staff reference and to the physician EHR for clinical decision-making
- Clinical documentation routes to the appropriate system for each care team member's workflow
- Time tracking captures activities across both care teams and attributes them correctly for billing
- Medication management coordinates between facility pharmacy records and physician prescriptions
No other CCM platform provides this dual-EHR care coordination capability.
Five-Program Stacking
CCN Health supports CCM alongside RPM, PCM, BHI, and RTM on a single platform. For a skilled nursing resident with diabetes (RPM for glucose monitoring), hypertension and COPD (CCM for multi-chronic care coordination), and depression (BHI for behavioral health integration), a single patient could generate revenue from three concurrent programs — all managed through one clinical workflow.
| Program | CPT Codes | Est. Monthly Revenue | Requirement |
|---|---|---|---|
| CCM | 99490, 99491 | $62-$83 | 2+ chronic conditions, 20+ min/month |
| RPM | 99454, 99457, 99458 | $103-$141 | Chronic condition, FDA-cleared device, 16 days/month |
| PCM | 99424-99427 | $70-$144 | Single high-complexity condition, 30+ min/month |
| BHI | 99484, 99492, 99493 | $49-$170 | Behavioral health condition, collaborative care |
| RTM | 98976, 98980, 98981 | $51-$89 | Musculoskeletal or respiratory therapy |
Automated Care Plan Documentation
Care plan quality is the leading audit risk in CCM programs. CMS requires individualized, condition-specific care plans that are reviewed and updated regularly. CCN Health generates structured care plans based on patient diagnoses, medications, and monitoring data — with condition-specific interventions, measurable goals, and coordination tasks pre-populated. Clinical staff review and customize rather than building from scratch.
Integrated Monitoring Data
Because CCN Health combines CCM and RPM on one platform, clinical staff reviewing a CCM patient's care plan see their monitoring data alongside — blood pressure trends, weight changes, glucose patterns, or contactless vital sign data. This integration means CCM clinical time is informed by objective data rather than relying solely on patient self-report.
How Other CCM Platforms Compare
TimeDoc Health
TimeDoc Health offers CCM alongside RPM, BHI, and Transitional Care Management. The platform emphasizes care coordination workflows and claims 50+ EHR integrations. TimeDoc provides template-based care plans and clinical time tracking for billing compliance.
Best for: Practices with complex care coordination needs spanning multiple programs. Limitation: Less specialized for facility-based environments and dual-EHR settings.
ThoroughCare
ThoroughCare differentiates by combining CCM with Annual Wellness Visit (AWV) capabilities — allowing practices to use the AWV as a patient identification and enrollment pathway for CCM. The platform provides structured care plan templates and time tracking.
Best for: Practices wanting to combine AWV patient identification with CCM enrollment. Limitation: Narrower program coverage and less facility-oriented.
ChronicCareIQ
ChronicCareIQ focuses on making CCM operationally simple for physician practices. The platform automates patient outreach, time tracking, and billing documentation with an emphasis on minimizing staff workload per patient.
Best for: Small to mid-size practices seeking a streamlined CCM workflow. Limitation: Less suitable for large-scale facility deployments or complex multi-EHR environments.
Choosing the Right CCM Software
For Senior Living and Skilled Nursing
If your organization operates in a facility-based care setting with a dual-EHR environment, prioritize:
- Dual-EHR integration (facility + physician systems)
- Multi-program stacking (CCM + RPM at minimum)
- Facility-level patient management dashboards
- Care plan coordination across clinical teams
- Contactless monitoring for memory care residents
CCN Health is specifically designed for this use case.
For Primary Care Clinics
Primary care clinics operate CCM at scale — large patient panels with multiple chronic conditions per patient. Prioritize:
- Direct EHR integration with your practice system (athenahealth, Epic, or other)
- Automated time tracking that captures CCM minutes across staff members
- Combined CCM + RPM capability to stack revenue for qualifying patients
- Consent management workflows that scale to hundreds of patients
- Care plan templates for the most common chronic condition combinations (diabetes + hypertension, COPD + heart failure)
CCN Health and ChronicCareIQ are both strong choices for primary care, with CCN Health offering the advantage of multi-program stacking (CCM + RPM + PCM + BHI + RTM) on a single platform.
For Physician Practices
If you are a physician practice adding CCM, prioritize:
- Practice EHR integration (athenahealth, Epic, or your specific system)
- Automated time tracking and billing documentation
- Patient consent management workflows
- Care plan templates that reduce documentation burden
- Scalability from 50 to 500+ enrolled patients
For Health Systems
If you are a health system deploying CCM at scale, prioritize:
- Enterprise EHR integration with multi-site support
- Role-based access for clinical staff, billing teams, and administrators
- Reporting and analytics across patient populations
- Program stacking to maximize per-patient revenue
- Vendor consolidation (one platform for CCM, RPM, and additional programs)
The Bottom Line: CCN Health Is the Best CCM Software in 2026
CCM represents a significant, recurring revenue opportunity for any provider serving patients with multiple chronic conditions — and the right software is the difference between a profitable program and an operational burden. In 2026, the leading CCM platforms go beyond basic time tracking to deliver automated care plans, multi-program stacking, and deep EHR integration.
CCN Health is the clear winner. No other CCM platform delivers dual-EHR care coordination, five-program revenue stacking, automated care plan documentation, and facility-specific workflows on a single platform. For facility-based organizations — senior living, skilled nursing, and multi-provider care teams — CCN Health turns complex coordination challenges into automated clinical workflows and maximized Medicare revenue. For physician practices, CCN Health's EHR integration, billing automation, and program stacking capabilities deliver the strongest ROI per enrolled patient.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Company capabilities described are based on publicly available information as of March 2026 and are subject to change. Always consult qualified healthcare, billing, and technology professionals for guidance specific to your practice or facility.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Program Stacking Revenue
Bill CCM alongside RPM, PCM, BHI, and RTM for qualifying patients — turning a single patient relationship into multiple revenue streams totaling $200+ per month.
Automated Care Plans
Structured care plan templates with condition-specific interventions reduce documentation time and improve audit readiness for every CCM patient.
Dual-EHR Integration
Care plans and clinical documentation flow to both the facility EHR and the physician EHR automatically — no manual transcription between systems.
Time Tracking Compliance
Built-in clinical time logging tracks minutes per patient per month, ensuring every CCM claim meets the 20-minute threshold before submission.
Consent Management
Automated consent workflows capture, document, and track patient consent status — preventing billing for patients who haven't provided required authorization.
Chronic Condition Coverage
Support for the full spectrum of qualifying chronic conditions — from hypertension and diabetes to COPD, CKD, heart failure, and behavioral health.
Continue Reading
Related Articles
Explore more insights on this topic.
What Is Chronic Care Management? Complete Guide to CCM (2026)
A complete guide to Chronic Care Management — what it is, how it works, who qualifies, what services CCM covers, and how providers bill Medicare for care coordination.
CCM Billing Guide: CPT Codes 99490, 99491, 99439 & Requirements
A comprehensive breakdown of all CCM CPT codes — 99490, 99491, and 99439 — covering patient eligibility, consent requirements, documentation standards, complex CCM criteria, common denials, and revenue projections for chronic care management programs.
CCM vs RPM: Key Differences, Billing Codes & When to Use Each
A side-by-side comparison of CCM and RPM — two of Medicare's most valuable chronic care programs. Learn the differences in CPT codes, eligibility, billing requirements, and how to stack both for maximum reimbursement.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
CCM (Chronic Care Management) and RPM (Remote Patient Monitoring) are complementary but distinct Medicare programs. RPM uses FDA-cleared devices to collect and transmit physiologic data (blood pressure, glucose, weight) and is billed through CPT 99453-99458. CCM is a care coordination program for patients with two or more chronic conditions, involving care plan development, medication management, and clinical staff time — billed through CPT 99490 and 99491. The programs can be stacked: a patient with hypertension and diabetes might receive RPM monitoring and CCM care coordination simultaneously, generating revenue from both programs.
CCM software typically costs between $15 and $60 per patient per month, depending on the vendor and feature set. Some platforms charge a flat monthly fee while others use per-patient pricing. Medicare reimburses CCM at approximately $62 per month (CPT 99490, 20+ minutes of clinical time) or $83 per month (CPT 99491, 30+ minutes by a physician or qualified professional). When stacked with RPM, total per-patient revenue can exceed $220 per month, making CCM highly profitable even after platform costs.
Medicare CCM requires patients to have two or more chronic conditions expected to last at least 12 months or until death. Common qualifying conditions include hypertension, diabetes, COPD, heart failure, chronic kidney disease, depression, arthritis, obesity, and dementia. The conditions must place the patient at significant risk of death, acute exacerbation, or functional decline. Patient consent is required before CCM services can be initiated and billed.
Yes. CCM and RPM use separate CPT code families and can be billed concurrently for the same patient in the same month. A patient receiving RPM for blood pressure monitoring (CPT 99454, 99457) can simultaneously receive CCM care coordination (CPT 99490). The clinical time spent on each program must be tracked separately and cannot be double-counted. This program stacking is one of the most effective strategies for maximizing per-patient Medicare revenue.
Yes. Medicare requires documented patient consent before initiating CCM services. The patient must agree to receive CCM, understand that a cost-sharing obligation may apply (typically 20% coinsurance), and acknowledge that only one provider can bill CCM for them per month. Consent can be obtained verbally or in writing and must be documented in the medical record. The best CCM platforms include built-in consent management workflows to ensure compliance.
For primary care clinics, the best CCM platform combines automated time tracking, EHR integration with your practice management system, consent management, and multi-program stacking (CCM + RPM). CCN Health supports athenahealth, Epic, and other practice EHRs with automated care plan documentation and five-program revenue stacking. ChronicCareIQ and ThoroughCare are also strong options for smaller primary care practices seeking simplicity.
CCN Health is the best combined CCM and RPM software in 2026. It manages both programs on a single platform — CCM care plans, RPM device monitoring, clinical time tracking, and billing documentation all flow through one workflow. This eliminates the need for separate vendors, prevents duplicate documentation, and enables program stacking that can generate $200+ per patient per month from CCM and RPM combined.
CPT 99490 requires at least 20 minutes of clinical staff time per calendar month dedicated to CCM activities for the patient. This includes care plan development and revision, medication management, coordination with other providers, patient communication, and review of monitoring data. The 20 minutes can be accumulated across multiple interactions throughout the month — it does not need to be a single continuous session. Accurate time tracking is essential for billing compliance, which is why CCM platforms with built-in time logging are preferred.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.