Program Stacking
RPM + BHI.
CMS allows concurrent billing of RPM and BHI for the same patient in the same calendar month. This combination addresses the intersection of chronic physical conditions and behavioral health — a pairing that affects millions of Medicare beneficiaries. Combined estimated revenue reaches $210–300 per patient per month while delivering whole-person care.
Side by Side
Feature comparison.
Analysis
Key considerations.
Different data domains — physiologic vs behavioral
RPM collects objective physiologic data from medical devices — blood pressure readings, weight trends, glucose levels, SpO2 values. BHI tracks behavioral health through validated screening tools (PHQ-9, GAD-7), care manager interactions, and psychiatric consultation notes. The data types are completely distinct, which is why CMS permits concurrent billing.
Time must be tracked separately for each program
Clinical time spent reviewing RPM device data and responding to physiologic alerts cannot count toward BHI. Similarly, time spent on behavioral health assessments, care management, and psychiatric consultation counts only toward BHI codes. Each program requires independent time documentation.
Combined care addresses the depression-chronic disease cycle
Research consistently shows that depression worsens chronic disease outcomes and that uncontrolled chronic conditions worsen depression. RPM catches physiologic deterioration that may signal behavioral health decline (e.g., rising blood pressure during a depressive episode), while BHI interventions improve medication adherence and self-management behaviors.
BHI adds revenue with minimal device cost
Unlike RPM, BHI does not require any monitoring device — it is assessment-based and care-coordination-based. Adding BHI to an existing RPM patient generates an additional ~$50–80/month (or more with CoCM codes) without additional device procurement or logistics costs.
Guidance
When to stack.
Stack RPM + BHI when
The patient has a chronic physical condition requiring device monitoring AND a co-occurring behavioral health condition. Common combinations include diabetes + depression (glucose monitoring + BHI), heart failure + anxiety (weight monitoring + BHI), hypertension + PTSD (BP monitoring + BHI), or COPD + substance use disorder (SpO2 monitoring + BHI).
Do not stack when
The patient does not have a diagnosed behavioral health condition — BHI requires a qualifying behavioral health diagnosis. Do not add BHI solely for revenue purposes without genuine clinical need. Also avoid stacking if the practice lacks a behavioral health care manager or psychiatric consultant, as inadequate BHI delivery risks audit exposure.
Ideal patient profiles
The strongest candidates are patients with diabetes and depression (the most studied comorbidity, affecting ~25% of diabetes patients), heart failure with anxiety (common post-hospitalization), chronic pain conditions with co-occurring depression, or elderly patients with multiple chronic conditions and adjustment disorders related to declining health.
FAQ
Common questions.
Can you bill RPM and BHI for the same patient in the same month?
Yes. CMS permits concurrent billing of RPM and BHI for the same patient in the same calendar month. The programs address different clinical domains — RPM covers physiologic monitoring while BHI covers behavioral health management. Time must be tracked independently for each program.
How much revenue can RPM + BHI generate combined?
Estimated combined revenue ranges from $210–300+ per patient per month. RPM contributes ~$160–220 (99453, 99454, 99445, 99457, 99470, 99458) and BHI contributes ~$50–80 (99484). Revenue can be higher if CoCM codes (99492–99494) are used instead of or in addition to general BHI.
Does BHI require a separate consent from RPM?
Yes. Each program requires independent patient consent. The RPM consent covers device monitoring and data transmission. The BHI consent covers behavioral health screening, care management services, and if applicable, involvement of a psychiatric consultant in the patient's care.
What behavioral health conditions qualify for BHI alongside RPM?
Qualifying behavioral health conditions include major depressive disorder, generalized anxiety disorder, substance use disorders, PTSD, bipolar disorder, and adjustment disorders. The condition must be clinically documented and actively managed through the BHI program — not simply listed as a historical diagnosis.
Do you need a psychiatrist to bill BHI with RPM?
For the general BHI code (99484), a psychiatric consultant is not strictly required — a behavioral health care manager can deliver services. However, if using CoCM codes (99492–99494), a consulting psychiatrist must be part of the care team. Many practices start with 99484 and add CoCM as their behavioral health team matures.
Quick Answer
The short version.
Yes, RPM and BHI can be billed together for the same patient in the same month. CMS permits concurrent billing because the programs address different clinical domains — RPM covers physiologic device monitoring while BHI covers behavioral health management. Combined estimated revenue reaches $210–300+ per patient per month, making this an effective stacking strategy for patients with chronic physical conditions and co-occurring depression, anxiety, or other behavioral health diagnoses.
More Comparisons
Also compare.
CCM vs RPM
Compare Chronic Care Management (CCM) and Remote Patient Monitoring (RPM): billing codes, patient eligibility, reimbursement, and when to use each.
CGM vs Glucose Meter
Compare continuous glucose monitors (CGMs) and traditional glucose meters for remote patient monitoring: data frequency, cost, patient experience, and clinical use cases.
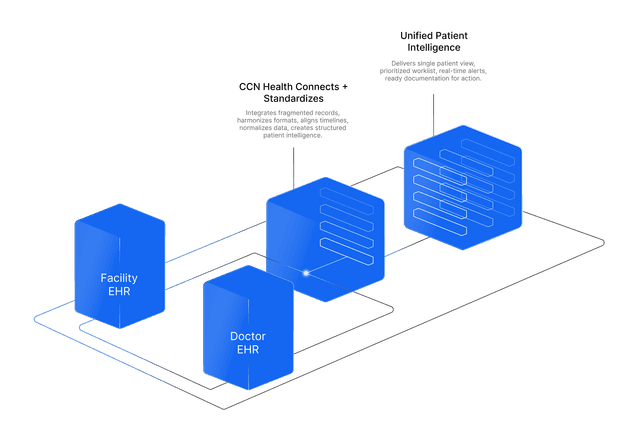
Facility EHR vs Practice EHR
Compare facility EHRs (PointClickCare, ALIS) with practice EHRs (athenahealth, Epic) for RPM integration: workflows, data flow, and implementation considerations.
RPM vs RTM
Compare Remote Patient Monitoring (RPM) and Remote Therapeutic Monitoring (RTM): CPT codes, eligible conditions, device requirements, and when to use each program.
BHI vs CCM
Compare Behavioral Health Integration (BHI) and Chronic Care Management (CCM): eligibility, billing codes, clinical workflows, and when to combine both programs.
RPM + CCM
Learn how to combine RPM and CCM for the same patient to maximize revenue and clinical outcomes. Requirements, billing rules, and implementation best practices.
CCM + BHI
CCM + BHI combined stacking for patients with chronic physical and behavioral health conditions. Billing requirements and revenue potential.
RPM + RTM
RPM + RTM combined stacking for patients with physiologic and therapeutic monitoring needs. Billing restrictions, revenue potential, and compliance.
RPM + PCM
Learn how to combine RPM and PCM for patients with a single complex chronic condition. Billing rules, revenue stacking, and key difference from CCM.
CCM + RTM
CCM + RTM combined stacking for the same patient. Billing rules, revenue estimates, eligible patient profiles, and compliance requirements.
CCM + PCM
CCM and PCM cannot be billed for the same patient in the same month. Why they are mutually exclusive, how to choose, and when to switch.
BHI + RTM
BHI + RTM combined stacking for the same patient. Billing rules, revenue estimates, and implementation guidance for behavioral and therapeutic care.
PCM + RTM
Learn how to combine Principal Care Management (PCM) and Remote Therapeutic Monitoring (RTM) for the same patient. Billing rules, eligible conditions, revenue estimates, and implementation best practices.
Cellular vs Bluetooth
Compare cellular and Bluetooth blood pressure monitors for remote patient monitoring: data reliability, patient experience, connectivity, and clinical outcomes.
Contactless (Radar) vs Wearable Devices
Compare radar-based contactless monitoring with traditional wearable RPM devices: patient experience, data types, compliance, and ideal care settings.