Guides
RPM for IDNs: Scaling Remote Patient Monitoring Across Facilities
A strategic guide for Integrated Delivery Networks deploying RPM across multiple care settings — from SNFs and assisted living to home health — with centralized clinical oversight, standardized protocols, and consolidated billing.
Integrated Delivery Networks (IDNs) scale RPM across facilities by deploying a unified platform with centralized clinical oversight, standardized monitoring protocols, and consolidated billing across all sites. The key challenges — vendor fragmentation, inconsistent alert thresholds, and data silos between facility EHRs — are solved by selecting an RPM partner that supports multi-site dashboards, dual-EHR integration, and enterprise-level reporting from a single platform.
The IDN RPM Challenge
Integrated Delivery Networks sit at the intersection of healthcare's greatest RPM opportunity and its most complex operational challenge. An IDN operating skilled nursing facilities, assisted living communities, and home health agencies under one umbrella has hundreds or thousands of patients with chronic conditions across multiple sites — all potentially eligible for Remote Patient Monitoring. The revenue opportunity is enormous. The implementation complexity is equally significant.
The fundamental problem is not whether RPM works. Single-facility RPM deployments have proven their clinical and financial value across care settings. The problem is what happens when an IDN tries to scale RPM from one facility to five, ten, or twenty — and discovers that each site has different devices, different alert thresholds, different EHR systems, and different billing workflows. Vendor fragmentation turns a revenue opportunity into an operational burden.
This guide covers how IDNs deploy RPM as a true enterprise capability — with centralized oversight, standardized clinical protocols, and consolidated billing — rather than a collection of independent facility programs.
Why Single-Facility RPM Models Break at IDN Scale
Vendor Fragmentation
When IDNs allow individual facilities to select their own RPM vendors, the network ends up with a patchwork of platforms. One skilled nursing facility uses Vendor A. An assisted living community across town uses Vendor B. The home health division uses Vendor C. Each platform has its own dashboard, its own alert logic, its own device ecosystem, and its own billing process.
Network leadership has no unified view of RPM performance. Clinical protocols differ between sites. A patient transitioning from the SNF to home health loses monitoring continuity entirely — their data lives in two separate, non-communicating systems. And the organization is paying multiple platform fees, managing multiple vendor relationships, and duplicating administrative overhead at every site.
Data Silos Between Facilities
IDN facilities commonly operate on different EHR systems. Skilled nursing facilities may run on PointClickCare. Assisted living communities may use ALIS or MatrixCare. Physician practices within the network may be on athenahealth or Epic. Each EHR integration is a separate technical project when RPM vendors operate independently at each site.
The clinical cost is significant. When a resident's RPM data is trapped in one facility's system, clinicians at other network facilities cannot access trends, baselines, or historical alerts. Care transitions — which are precisely the moments when monitoring data is most valuable — become blind handoffs.
Inconsistent Clinical Protocols
Without enterprise-level standardization, each facility develops its own RPM protocols. Blood pressure alert thresholds differ between the SNF and the assisted living community. Escalation pathways vary. Documentation standards are inconsistent. Device types and connectivity requirements change from site to site. This variability creates clinical risk and makes network-level quality measurement impossible.
Revenue Leakage from Decentralized Billing
Fragmented RPM programs leak revenue in multiple ways. Individual facilities miss program stacking opportunities because they lack visibility into which patients qualify for CCM, PCM, or BHI alongside RPM. Billing compliance varies by site — some facilities underbill because they do not track clinical time accurately, while others face audit risk from inconsistent documentation. And administrative duplication across multiple billing workflows increases cost per claim.
The Enterprise RPM Architecture for IDNs
Centralized Platform, Distributed Execution
The most effective IDN RPM architecture uses a single platform deployed across all facilities with centralized configuration and distributed day-to-day execution. In practice, this means:
- One RPM platform serves every facility in the network, regardless of care setting or EHR system
- Network-level administrators configure alert thresholds, device standards, escalation protocols, and billing rules
- Facility-level staff execute daily monitoring workflows within the standardized framework — taking readings, managing devices, and responding to alerts according to network protocols
- Centralized clinical monitoring teams provide oversight across all sites, triaging alerts and ensuring consistent clinical responses
This model preserves each facility's operational autonomy while eliminating the variability that undermines clinical quality and financial performance.
Multi-EHR Integration Layer
An IDN RPM platform must integrate with every EHR system in the network simultaneously. This is not a single integration project — it is an ongoing multi-system capability.
| Care Setting | Common EHR | Integration Requirement |
|---|---|---|
| Skilled Nursing | PointClickCare | RPM data in resident clinical record, nursing documentation |
| Assisted Living | ALIS, MatrixCare | RPM readings mapped to health records, care plan updates |
| Home Health | Various | Remote device data linked to patient episodes |
| Physician Practices | athenahealth, Epic | Monitoring data in physician workflow, order management |
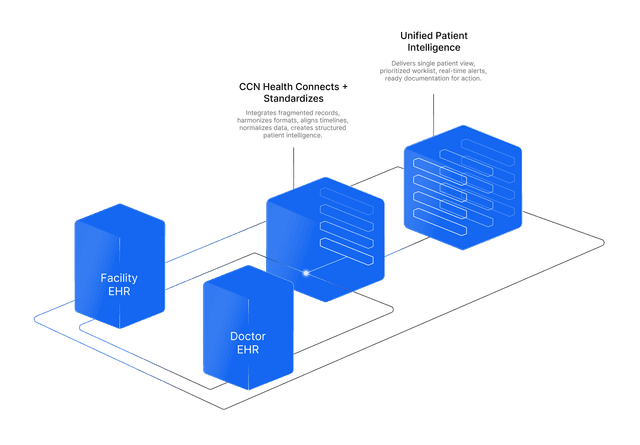
CCN Health's dual-EHR architecture is designed for exactly this scenario — bridging facility EHRs and practice EHRs within a single monitoring platform. RPM data flows into each facility's clinical record without requiring facilities to change their EHR system, while network leadership accesses all data through a centralized dashboard.
Centralized Clinical Oversight Dashboard
The network-level dashboard is the command center for IDN RPM operations. It provides:
- Network-wide patient census — Total enrolled patients, active devices, and compliance metrics across all facilities
- Cross-facility alert queue — Prioritized alerts from every site in a single view, triaged by clinical severity rather than facility of origin
- Facility performance comparison — Enrollment rates, compliance rates, alert response times, and revenue per patient by site
- Transition tracking — Patients moving between facilities with continuity of monitoring data and care plans
- Population health views — Condition-specific cohort analysis, trending vitals across the network's patient population
Facility-level staff see their own patients and alerts. Network clinical directors see everything.
Standardizing RPM Protocols Across the Network
Alert Thresholds and Escalation Pathways
One of the highest-impact actions an IDN can take is standardizing RPM alert thresholds and escalation pathways across all facilities. This means every site uses the same clinical criteria for what constitutes an alert-worthy reading and the same escalation sequence for clinical response.
Standardized thresholds example (blood pressure):
| Alert Level | Systolic | Diastolic | Response |
|---|---|---|---|
| Watch | 140-159 | 90-99 | Clinical review within 4 hours |
| Urgent | 160-179 | 100-109 | Clinical contact within 1 hour |
| Critical | 180+ | 110+ | Immediate escalation to physician |
Without standardization, one facility might flag a systolic reading of 150 as critical while another ignores it entirely. Standardized thresholds ensure consistent clinical response regardless of which facility the patient resides in.
Device and Connectivity Standards
IDNs should mandate a standard device ecosystem across all facilities:
- Cellular-only connectivity — Eliminates Wi-Fi and Bluetooth dependency across all settings
- Approved device list — Standardized blood pressure monitors, weight scales, pulse oximeters, and contactless monitors used at every site
- Device management protocols — Consistent charging, assignment, replacement, and troubleshooting workflows
- Contactless monitoring standards — Consistent deployment criteria for contactless devices in memory care and high-acuity settings
Device standardization reduces procurement costs, simplifies staff training (staff transferring between facilities already know the equipment), and ensures data comparability across sites.
Documentation and Compliance Standards
Enterprise RPM documentation standards ensure every facility captures the clinical time, patient interactions, and monitoring activities required for billing compliance:
- Time tracking rules — Consistent methods for documenting CPT 99457 and 99458 clinical time across all sites
- Care plan integration — Standardized documentation of how RPM data informs clinical decision-making
- Consent management — Network-wide consent workflows with centralized tracking of patient authorization status
- Audit preparation — Uniform documentation that meets CMS requirements at every facility
The Financial Case for Enterprise RPM
Economies of Scale
IDN-level RPM deployment reduces per-patient costs compared to independent facility programs:
- Platform costs — Enterprise licensing reduces per-site or per-patient platform fees
- Clinical monitoring — Centralized monitoring teams serve multiple facilities, reducing per-site staffing requirements
- Device procurement — Volume purchasing reduces per-device costs across the network
- Training and implementation — Standardized onboarding processes become more efficient with each additional facility
- Vendor management — One vendor relationship replaces three, five, or ten
Program Stacking at Network Scale
Program stacking — billing RPM alongside CCM, PCM, BHI, and RTM — is where IDN RPM economics become truly compelling. A centralized platform identifies stacking opportunities across the entire patient population rather than leaving it to individual facility staff to recognize qualifying patients.
| Program Stack | Est. Monthly Revenue/Patient | IDN Advantage |
|---|---|---|
| RPM only | $103-$141 | Scale across hundreds of patients |
| RPM + CCM | $165-$224 | Centralized care plan coordination |
| RPM + CCM + PCM | $235-$368 | Automated program qualification |
| RPM + CCM + BHI | $214-$394 | Behavioral health integration across sites |
An IDN with 500 eligible patients across five facilities, averaging RPM + CCM stacking, generates an estimated $80,000-$112,000 in monthly Medicare reimbursement — revenue that fragmented, single-facility programs systematically undercapture.
Population Health and Value-Based Performance
Network-wide RPM data creates a population health asset that individual facilities cannot generate independently. Aggregated monitoring data across the IDN reveals:
- Condition prevalence patterns — Hypertension rates, diabetes management effectiveness, and COPD exacerbation frequency across the network
- High-risk patient identification — Patients trending toward hospitalization based on vital sign patterns, identified early enough for intervention
- Care transition outcomes — How effectively patients maintain health metrics when moving between IDN facilities
- Facility-level quality benchmarking — Which sites achieve the best clinical outcomes and what practices drive those results
For IDNs participating in value-based contracts, ACOs, or bundled payment programs, this data directly supports quality measure reporting and shared savings calculations.
Implementation: Phased Rollout for IDNs
Phase 1: Network Assessment and Platform Selection (Weeks 1-4)
Facility readiness audit — Assess each facility across four dimensions: EHR system and integration readiness, staff capacity and willingness, patient population (chronic condition prevalence), and existing RPM activity to consolidate.
Pilot facility selection — Choose the facility with the highest readiness score. Ideal pilot characteristics include:
- High chronic condition prevalence in the resident/patient census
- Engaged facility leadership and clinical champions
- EHR system already supported by the selected RPM platform
- Manageable size (80-150 beds) for workflow validation
Enterprise protocol development — Before launching anywhere, develop the network-wide standards: alert thresholds, escalation pathways, device list, documentation requirements, and billing workflows. These standards deploy with the pilot and carry forward to every subsequent facility.
Phase 2: Pilot Facility Launch (Weeks 5-8)
Launch the pilot facility using the same phased approach recommended for single-facility deployments — but with enterprise-level configuration:
- Configure EHR integration for the pilot facility's specific system
- Deploy standardized devices and train staff on network protocols
- Activate the centralized monitoring dashboard with the pilot facility's patients
- Validate billing workflows through the consolidated billing process
- Document every workflow adjustment for application to subsequent facilities
The pilot validates not just facility-level operations but the entire enterprise infrastructure: centralized dashboard, multi-facility alert routing, enterprise billing, and cross-site reporting.
Phase 3: Controlled Expansion (Months 3-4)
Expand to the next 2-3 facilities simultaneously, applying lessons from the pilot:
- Each facility follows the standardized onboarding playbook
- EHR integrations proceed in parallel (different facilities, different EHR systems)
- Staff training uses materials refined during the pilot
- Centralized monitoring absorbs new facility patient loads incrementally
- Billing workflows scale with the new patient census
Phase 4: Full Network Deployment (Months 4-6)
Continue expansion in waves until all network facilities are live. By this stage, the onboarding process is repeatable and efficient. The centralized monitoring team, enterprise dashboard, and billing infrastructure are proven at scale.
Ongoing Optimization
Enterprise RPM is not a one-time implementation — it is an ongoing capability that improves over time:
- Monthly performance reviews — Compare facility metrics and identify underperforming sites for targeted intervention
- Protocol refinement — Adjust alert thresholds and escalation pathways based on accumulated outcome data
- Program expansion — Add CCM, PCM, and BHI stacking as the RPM foundation matures
- New facility onboarding — As the IDN acquires or opens new facilities, RPM deployment follows the established playbook
Common Mistakes IDNs Make with RPM
Allowing Facility-Level Vendor Selection
The single most expensive mistake is allowing individual facilities to choose their own RPM vendors. The short-term path of least resistance creates long-term vendor fragmentation, data silos, and operational inefficiency that costs far more to unwind than a coordinated enterprise deployment costs to execute.
Deploying Without Standardized Protocols
Launching RPM across multiple facilities without network-wide clinical standards creates inconsistency that undermines clinical quality and complicates billing compliance. Standardize protocols before deploying to the first facility — not after discovering variability at the fifth.
Underestimating EHR Integration Complexity
IDNs with mixed EHR environments (PointClickCare at some sites, ALIS at others, athenahealth for affiliated practices) need an RPM partner with proven multi-EHR integration capabilities. Treating each site's EHR integration as an independent project leads to delays, inconsistencies, and ongoing maintenance burden.
Skipping the Pilot
The pressure to demonstrate network-wide results quickly tempts IDN leadership to launch at all facilities simultaneously. This almost always produces workflow failures, staff burnout, and clinical risk. A 4-week pilot at a single facility costs minimal time and saves months of remediation.
Ignoring Care Transitions
Patients move between IDN facilities — from the SNF to assisted living, from assisted living to home health. If the RPM platform does not maintain monitoring continuity across transitions, the IDN loses the primary clinical advantage of operating as an integrated network. Care transitions are where monitoring data is most valuable and where fragmented systems fail most visibly.
Choosing the Right RPM Partner for IDN Scale
When evaluating RPM platforms for enterprise deployment, IDNs should assess:
| Capability | Why It Matters for IDNs |
|---|---|
| Multi-site dashboard | Network-level visibility into all facilities from a single interface |
| Multi-EHR integration | Bridge facility EHRs (PCC, ALIS, MatrixCare) and practice EHRs (athenahealth, Epic) |
| Standardized protocol engine | Configure alert thresholds, escalation pathways, and device standards at the network level |
| Program stacking | RPM + CCM + PCM + BHI + RTM on one platform to maximize per-patient revenue |
| Population health analytics | Network-wide cohort analysis, trending, and outcome measurement |
| Transition continuity | Maintain monitoring data and care plans as patients move between facilities |
| Enterprise billing | Consolidated billing workflows across all sites with centralized revenue tracking |
| Scalable architecture | Add facilities, programs, and patient volume without platform limitations |
CCN Health is purpose-built for this use case — with dual-EHR integration across facility and practice EHR systems, multi-site clinical dashboards, five-program stacking, and enterprise-level configuration that supports IDNs operating across mixed care settings.
Conclusion
For IDNs, the question is not whether to offer RPM — it is whether to do it as a fragmented collection of facility-level programs or as a coordinated enterprise capability. The financial and clinical case for enterprise RPM is compelling: economies of scale reduce per-patient costs, centralized monitoring improves clinical consistency, consolidated billing captures revenue that fragmented operations miss, and population health analytics unlock insights invisible to individual facilities.
The implementation path is proven: standardize protocols first, validate with a single-facility pilot, expand in controlled waves, and optimize continuously. The IDNs that treat RPM as enterprise infrastructure — not a facility-level add-on — will capture the full clinical and financial value of remote monitoring at scale.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Always consult qualified healthcare, billing, and technology professionals for guidance specific to your organization.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Centralized Clinical Oversight
Monitor patients across every facility in the network from a single dashboard — with role-based views for network leadership, clinical teams, and facility staff.
Standardized Protocols
Consistent alert thresholds, escalation pathways, and device configurations eliminate dangerous clinical variability across facilities.
Consolidated Billing
Enterprise billing workflows capture RPM, CCM, and PCM revenue across all sites — eliminating the revenue leakage that fragmented billing creates.
Multi-EHR Integration
Bridge facility EHRs (PointClickCare, ALIS, MatrixCare) and practice EHRs (athenahealth, Epic) across every site in the network from a single RPM platform.
Population Health Analytics
Network-wide monitoring data reveals condition trends, high-risk cohorts, and intervention opportunities invisible to individual facility dashboards.
Scalable Architecture
Add facilities, device types, and Medicare programs without platform changes — the same infrastructure supports 3 sites or 30.
Continue Reading
Related Articles
Explore more insights on this topic.
Best Remote Patient Monitoring Companies, Platforms & Vendors (2026)
A side-by-side comparison of the leading remote patient monitoring companies in 2026 — covering programs, devices, EHR integrations, and care settings — with an in-depth look at what sets CCN Health apart.
Best RPM Software for Enterprise & Health Systems in 2026
A head-to-head comparison of the best enterprise RPM platforms in 2026 — covering multi-site management, EHR integrations, program stacking, role-based access, and organizational scalability for health systems, IDNs, and multi-facility operators.
How to Launch RPM in Senior Living Facilities
A practical implementation guide for launching Remote Patient Monitoring in senior living facilities, covering census-based enrollment strategies, facility EHR integration with PointClickCare and ALIS, device selection for memory care and assisted living, and staff workflow design.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
An Integrated Delivery Network is a healthcare organization that operates multiple care settings — such as skilled nursing facilities, assisted living communities, home health agencies, and physician practices — under a single organizational umbrella. In the context of RPM, an IDN deploys remote monitoring across these settings with centralized oversight, standardized protocols, and consolidated billing rather than allowing each facility to operate an independent RPM program with different vendors, devices, and clinical workflows.
When individual facilities within an IDN select their own RPM vendors, the network ends up with multiple platforms that do not communicate with each other. Clinical data is siloed — a patient transitioning from a skilled nursing facility to home health loses monitoring continuity. Alert thresholds differ between sites. Device types and connectivity requirements vary. Billing is duplicated across vendors. And network leadership has no unified view of RPM performance, patient outcomes, or revenue across the organization. A single enterprise RPM platform eliminates all of these issues.
A centralized RPM dashboard aggregates patient monitoring data from all facilities in the IDN into a single interface. Network-level clinical staff can view alerts, compliance metrics, and patient trends across every site. Facility-level staff see only their own residents or patients. Role-based access controls ensure appropriate visibility at each organizational level. The dashboard enables network leadership to compare facility performance, identify outliers, and enforce standardized clinical protocols — capabilities impossible when each facility runs its own independent RPM system.
Yes, but only if the RPM platform supports multi-EHR integration. IDNs commonly operate mixed EHR environments — skilled nursing facilities on PointClickCare, assisted living on ALIS, and physician practices on athenahealth or Epic. The RPM platform must integrate with each facility's EHR independently while feeding all monitoring data into a centralized clinical and billing layer. CCN Health's dual-EHR architecture is designed specifically for this scenario, bridging facility and practice EHR systems across the network.
IDN-scale RPM generates disproportionately higher ROI than single-facility deployments for several reasons. Economies of scale reduce per-device and per-patient platform costs. Centralized clinical monitoring teams serve multiple facilities, reducing per-site staffing needs. Consolidated billing captures revenue missed by fragmented operations — particularly program stacking opportunities (RPM + CCM + PCM). Population health data across the network identifies high-risk patients earlier, reducing costly readmissions and emergency transfers. And standardized protocols improve clinical outcomes, which drives value-based contract performance.
A typical IDN RPM deployment takes 3 to 6 months from initial planning to full network coverage, depending on the number of facilities and EHR environments. Phase 1 (weeks 1-4) covers platform selection, protocol standardization, and pilot facility setup. Phase 2 (weeks 5-8) launches the pilot facility with full EHR integration and staff training. Phase 3 (months 3-6) expands to additional facilities in waves of 2-3 sites, applying lessons from each wave. Ongoing optimization continues after deployment as the network refines protocols, expands enrolled populations, and stacks additional programs.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.