business
How to Launch RPM in Senior Living Facilities
A practical implementation guide for launching Remote Patient Monitoring in senior living facilities, covering census-based enrollment strategies, facility EHR integration with PointClickCare and ALIS, device selection for memory care and assisted living, and staff workflow design.
To launch RPM in a senior living facility, follow a phased approach: (1) audit the resident census for qualifying chronic conditions and identify the initial unit or wing for pilot deployment, (2) select cellular-enabled devices appropriate for the care setting — contactless for memory care, staff-assisted for assisted living, (3) configure facility EHR integration with PointClickCare, ALIS, or MatrixCare, (4) train facility nursing staff on device management, reading workflows, and alert escalation, (5) enroll a pilot wing of 15-25 residents with family consent and physician orders, and (6) scale unit-by-unit across the facility. Senior living facilities typically achieve 40-70% enrollment rates and 80%+ 16-day compliance when readings are staff-assisted.
Why Senior Living RPM Is Different
Remote Patient Monitoring in senior living facilities operates under fundamentally different conditions than RPM in a physician practice. In a practice, you identify patients during office visits, hand them a device, and rely on them to take readings independently at home. In a senior living facility, the dynamics shift entirely.
Residents live on-site. Staff are present around the clock. The clinical record lives in a facility EHR — not a practice EHR. The ordering physician may be an external attending who visits weekly or a medical director who oversees the building. Enrollment is a census-level operation, not a one-patient-at-a-time process. And device selection must account for cognitive impairment, limited dexterity, shared living environments, and the absence of personal Wi-Fi networks.
These differences are not obstacles — they are actually advantages. Facility-based RPM programs consistently achieve higher compliance rates, better clinical engagement, and more predictable revenue than practice-based programs because staff can integrate readings into existing care routines. But realizing those advantages requires an implementation approach designed specifically for senior living environments.
Phase 1: Planning and Census Assessment (Weeks 1-2)
Audit the Resident Census
Start by analyzing your facility's resident census for RPM eligibility. Pull a report of all current residents and identify those with chronic conditions that benefit from physiologic monitoring:
- Hypertension — The most common starting condition; large eligible population, simple device (blood pressure monitor)
- Heart failure — Daily weight and blood pressure monitoring reduces readmission risk
- Diabetes — Blood glucose or continuous glucose monitoring for insulin-managed residents
- COPD — Pulse oximetry monitoring for residents with chronic respiratory conditions
- Fall risk — Contactless monitoring for residents at elevated fall risk, particularly in memory care
In a typical assisted living facility, 60-80% of residents have at least one chronic condition that qualifies for RPM. The goal is not to enroll every resident immediately — it is to understand the size and composition of your eligible population.
Select Your Pilot Unit
Rather than launching facility-wide, start with a single unit or wing. Choose a unit that:
- Has a high concentration of residents with qualifying conditions
- Is staffed by experienced nursing staff who can champion the program
- Has a manageable size (15-30 residents) for validating workflows
- Represents the care setting you plan to scale (assisted living, memory care, or skilled nursing)
A single-unit pilot allows you to validate every workflow element before expanding — device management, staff routines, physician communication, documentation, and billing.
Evaluate Device Requirements by Care Setting
Device selection in senior living depends heavily on the care environment:
Assisted Living — Most residents can participate in staff-assisted readings where a nurse or aide brings the device during morning rounds. Cellular blood pressure monitors and weight scales are the primary devices. Some higher-functioning residents may take independent readings in their rooms with cellular devices.
Memory Care — Residents cannot be expected to initiate readings or interact with devices independently. Contactless monitoring devices that use radar or sensor technology to track vitals, sleep patterns, and respiratory rate without resident interaction are ideal. For readings that require resident participation (blood pressure, weight), staff must perform the reading entirely.
Skilled Nursing — Nursing staff already take vitals as part of daily care routines. RPM adds automated data transmission from the device to the monitoring platform (and EHR) rather than manual charting. Cellular devices that transmit readings automatically eliminate the transcription step.
Across all settings: Cellular connectivity is mandatory. Residents do not have personal Wi-Fi networks, smartphones, or the ability to manage Bluetooth pairing. Every device must transmit data over cellular networks without any resident configuration.
Coordinate with Ordering Physicians
In senior living, the ordering physician structure differs from a standard practice:
- Skilled nursing — The attending physician or medical director typically orders RPM services. Work with the medical director to establish a standing protocol.
- Assisted living — Each resident's primary care physician may need to order individually. Develop a template order that external physicians can sign.
- Memory care — Orders may require coordination with the attending physician and family or legal representative.
Establish the physician order workflow before enrollment begins. Common approaches include: the medical director orders RPM for all qualifying residents, or individual attending physicians sign facility-provided order templates.
Phase 2: Configuration and EHR Integration (Weeks 2-3)
Configure Facility EHR Integration
The facility EHR is the primary clinical record in senior living. RPM data must flow into this system alongside ADL documentation, medication records, and nursing assessments.
Work with your RPM vendor and EHR team to establish integration with your facility system:
- PointClickCare — The dominant EHR in skilled nursing and many assisted living facilities. Integration enables RPM readings to appear in the resident's clinical record and progress notes.
- ALIS — Purpose-built for assisted living and memory care. RPM integration maps readings to the resident's health record within the ALIS platform.
- MatrixCare — Used across senior living settings. Supports RPM data integration through its clinical documentation framework.
Integration scope typically includes: incoming vital sign data from RPM devices, alert notifications within the EHR, and trend data accessible to nursing staff reviewing the resident's chart. Most facility EHR integrations take 2-3 business days to configure and validate.
Design Staff Workflows for Device Management
Facility RPM involves managing devices at scale. A 100-bed facility with 60% enrollment means 60+ active devices that need daily management. Design workflows for:
- Morning rounds integration — Incorporate blood pressure and weight readings into existing vitals routines. Staff bring devices to each resident's room during morning care.
- Device charging and storage — Designate a charging station at each nursing station. Establish overnight charging protocols so devices are ready for morning rounds.
- Device assignment tracking — Maintain a log of which device is assigned to which resident. Cellular devices are typically assigned to individual residents; shared devices need a clear checkout/return process.
- Troubleshooting protocols — Define what staff should do when a device fails to transmit, displays an error, or a resident reports a problem. Include replacement procedures.
- Contactless device management — For memory care contactless monitors, define installation locations, maintenance schedules, and what staff should do when the device is inadvertently moved or unplugged.
Set Up Clinical Monitoring Workflows
Define how RPM data will be monitored and acted upon:
- Who monitors — Will facility nursing staff review RPM dashboards, or will a centralized remote monitoring team handle data review? Many facilities use a hybrid model.
- Alert routing — Define alert thresholds for each vital sign type and the escalation path (staff nurse → charge nurse → medical director → attending physician).
- Documentation requirements — Establish how monitoring interactions are documented for CPT 99457/99458 billing alongside facility care documentation.
Phase 3: Staff Training (Week 3)
Train Nursing Staff on Device Operations
Every nursing staff member who will assist with readings needs hands-on training:
- How to operate each device type (blood pressure, weight scale, pulse oximeter, contactless monitor)
- How to confirm a successful reading and data transmission
- What to do when a reading fails to transmit
- How to replace a device that malfunctions
- How to manage the daily device charging routine
Train Clinical Staff on Monitoring and Documentation
Staff responsible for RPM data review need training on:
- Navigating the RPM monitoring dashboard
- Interpreting alerts and prioritizing clinical responses
- Documenting clinical time with date, duration, and activity descriptions
- The escalation protocol for out-of-range readings
- Communicating with attending physicians about RPM findings
Engage Families and Representatives
In senior living, families play a significant role in consent and engagement. Prepare a communication plan that:
- Explains the RPM program and its clinical benefits
- Addresses common family questions about privacy and data security
- Outlines the consent process (particularly for memory care residents whose legal representatives must consent)
- Provides a point of contact for ongoing questions
Phase 4: Pilot Launch (Weeks 3-5)
Enroll the Pilot Wing
Begin enrolling residents on your selected pilot unit. For each resident:
- Physician order — Obtain a signed order specifying the chronic condition and monitoring type
- Consent — Obtain consent from the resident or their legal representative (particularly important for memory care)
- Device assignment — Provision and assign the appropriate device(s) to the resident
- EHR documentation — Document the RPM enrollment in the resident's facility EHR record
- Platform activation — Activate the resident in the RPM monitoring platform with appropriate alert thresholds
Integrate into Daily Care Routines
The pilot period is about proving that RPM readings can be incorporated into existing staff routines without creating unsustainable workload. Focus on:
- Morning round timing — How long does it add to morning rounds to take RPM readings? Adjust scheduling if needed.
- Device logistics — Are devices charged and ready each morning? Is the charging workflow sustainable?
- Data flow validation — Are readings transmitting from devices to the RPM platform to the facility EHR?
- Staff feedback — Daily check-ins with nursing staff during the first week to identify friction points.
First-Week Validation
During the first week of your pilot, confirm:
- All enrolled residents have active devices transmitting data
- RPM readings appear in both the monitoring platform and facility EHR
- Alert thresholds are calibrated appropriately (not too sensitive, not too lax)
- Staff can complete RPM readings within their existing care routine
- Device charging workflow is functioning
- Clinical monitoring and time documentation are operational
Phase 5: Scale Across the Facility
Expand Unit by Unit
Once the pilot unit workflows are validated, expand systematically:
- Month 2 — Add a second unit or wing, applying lessons from the pilot
- Month 3 — Continue expanding, potentially adding new device types or care settings (e.g., extending from assisted living to memory care)
- Ongoing — Scale toward full facility coverage, incorporating new residents as they admit
Optimize for 16-Day Compliance
Staff-assisted readings in senior living facilities achieve significantly higher compliance than independent patient use. Target 80%+ 16-day compliance by:
- Incorporating RPM readings into the daily care routine (readings happen automatically as part of standard rounds)
- Tracking compliance by resident and unit on a weekly basis
- Addressing gaps immediately — if a resident misses readings for 2-3 days, investigate why
- Adjusting workflows for residents who are frequently off-unit (appointments, outings, hospitalizations)
Stack Complementary Programs
Senior living residents with multiple chronic conditions often qualify for additional programs:
- CCM — Most multi-chronic residents qualify for care coordination services alongside RPM
- BHI — Depression and anxiety are prevalent in senior living populations
- PCM — For residents with a single dominant chronic condition requiring intensive management
Program stacking in senior living can increase per-resident revenue from an estimated $120/month (RPM alone) to over $250/month for residents receiving RPM + CCM.
Common Mistakes in Senior Living RPM
Treating It Like Practice RPM
The biggest implementation error is applying a practice-based RPM model to a facility setting. Practice RPM relies on patients taking their own readings at home. Facility RPM is staff-driven, census-based, and integrated with existing care routines. The workflows, device selection, enrollment approach, and staffing model all differ.
Choosing Wi-Fi or Bluetooth Devices
Devices that require Wi-Fi networks or Bluetooth pairing to smartphones fail in senior living environments. Residents do not have personal Wi-Fi. They do not have smartphones (or cannot reliably operate them). Cellular-enabled devices that transmit data automatically are the only viable option.
Launching Facility-Wide Immediately
Facilities that try to enroll 100+ residents on day one overwhelm their nursing staff and create device management chaos. Start with a single unit, validate workflows, and then scale systematically.
Ignoring Device Management Logistics
Sixty devices need daily charging, assignment tracking, troubleshooting, and replacement. Facilities that do not plan for device logistics end up with dead batteries, lost devices, and frustrated staff. Establish a device management workflow before enrollment begins.
Not Engaging Families Early
In assisted living and memory care, family members influence (and sometimes control) consent decisions. Facilities that begin enrollment without a family communication plan face slow consent rates and pushback from uninformed family members.
Conclusion
Senior living facilities have a structural advantage for RPM that no other care setting can match: staff are present around the clock, residents are on-site, and care routines already include vital sign collection. The implementation challenge is not convincing patients to use devices independently — it is integrating RPM into existing facility workflows at scale.
A phased approach — starting with a single pilot unit, validating device logistics and staff workflows, and then expanding systematically — consistently produces better results than facility-wide launches. The financial opportunity is substantial: an estimated $120-160 per resident per month in RPM revenue alone, with the potential to exceed $250/month when stacking with CCM for qualifying residents.
Get Started
Ready to bring RPM to your senior living community? Talk to the CCN Health team for a customized implementation roadmap and platform walkthrough.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Always consult qualified healthcare and billing professionals for guidance specific to your facility.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Census-Based Revenue
Facility-wide enrollment generates predictable, recurring revenue across the resident census rather than depending on individual patient appointments.
Staff-Assisted Compliance
Facility staff incorporate device readings into daily care routines, achieving 80%+ 16-day compliance rates that independent patient use rarely matches.
Passive Memory Care Monitoring
Contactless and radar-based devices enable RPM for memory care residents who cannot independently operate traditional monitoring equipment.
Facility EHR Integration
RPM data flows directly into PointClickCare, ALIS, or MatrixCare — no manual transcription, no duplicate documentation, no workflow disruption.
Clinical Oversight at Scale
Centralized monitoring dashboards allow clinical staff to oversee 50-100+ residents from a single interface with automated alert prioritization.
Continue Reading
Related Articles
Explore more insights on this topic.
BHI Billing Guide: Behavioral Health Integration CPT Codes & Requirements
A detailed guide to Behavioral Health Integration billing — covering CPT codes 99484, 99492, and 99493, the Collaborative Care Model (CoCM), PHQ-9 and GAD-7 screening requirements, qualifying behavioral health conditions, and strategies for integrating BHI into primary care practice.
How to Bring RPM In-House: A 2027 Transition Playbook
CMS has proposed paying for RPM and RTM only when practice-employed clinical staff furnish the services, effective January 1, 2027 if finalized. For every practice running RPM on contracted staffing, that starts a clock. This playbook walks through the seven steps of a clean transition: mapping your exposure, hiring an employed team, choosing self-service software, and running a cutover month without a billing gap.
CCM Billing Guide: CPT Codes 99490, 99491, 99439 & Requirements
A comprehensive breakdown of all CCM CPT codes — 99490, 99491, and 99439 — covering patient eligibility, consent requirements, documentation standards, complex CCM criteria, common denials, and revenue projections for chronic care management programs.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
Senior living RPM differs in several key ways. Enrollment is census-based (working through the facility roster) rather than appointment-driven. Staff assist residents with device readings rather than relying on independent patient use. The facility EHR (PointClickCare, ALIS, MatrixCare) is the primary clinical record, requiring integration distinct from practice EHR systems. Device selection must account for cognitive impairment, limited dexterity, and shared living environments. And the ordering physician may be an external attending or medical director rather than an on-site provider, requiring coordination across organizational boundaries.
Memory care environments require devices that collect data passively or with minimal resident interaction. Contactless monitoring devices that use radar-based sensing to track vital signs, sleep patterns, and respiratory rate without any resident action are ideal. For blood pressure and weight, staff-assisted readings using cellular devices work when incorporated into existing care routines (e.g., morning vitals). Avoid any device requiring the resident to initiate readings, pair via Bluetooth, or interact with a smartphone app. Cellular connectivity is mandatory — memory care residents do not have personal Wi-Fi networks.
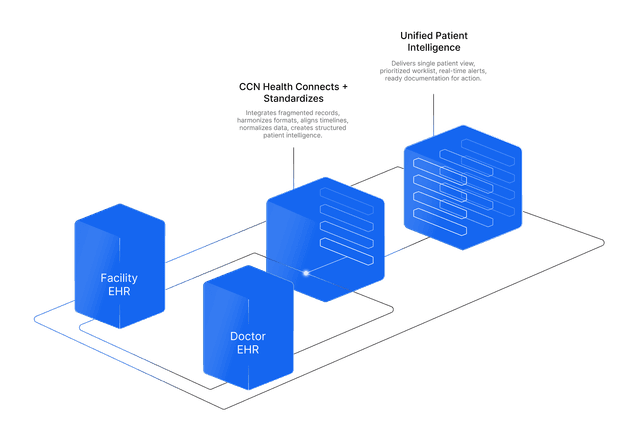
The major facility EHR systems that support RPM integration include PointClickCare (the dominant EHR in skilled nursing and many assisted living facilities), ALIS (focused on assisted living and memory care), and MatrixCare (used across senior living settings). Integration methods vary — HL7 feeds, FHIR APIs, or proprietary connectors. The integration ensures that RPM readings flow into the resident's clinical record alongside ADL documentation, medication records, and nursing notes. Most integrations take 2-3 business days to configure and validate.
In senior living, the ordering physician is often the resident's attending physician or the facility medical director, not a provider on staff at the facility. RPM orders must come from a physician with an established patient-provider relationship. Work with the medical director to establish a standing order protocol or template that attending physicians can sign. Some facilities designate the medical director as the ordering provider for all RPM services. Ensure that physician oversight and escalation procedures account for the off-site relationship — clinical monitoring staff need a clear pathway to reach the ordering physician when intervention is needed.
Enrollment rates vary by care setting and approach. Assisted living facilities typically achieve 40-70% resident participation when RPM is positioned as part of the care program and families are engaged in the consent process. Skilled nursing facilities can reach 60-80% because nursing staff control the care routine and can integrate device readings into daily workflows. Memory care enrollment depends on family or legal representative consent and typically ranges from 30-50%. The key factors are staff buy-in, family communication, and whether RPM is presented as an opt-out standard of care versus an opt-in add-on.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.