Guides
How RPM Reduces SNF Readmissions and Avoids VBP Penalties
73% of skilled nursing facilities face Value-Based Purchasing payment adjustments tied to hospital readmission rates. RPM provides early clinical intervention that keeps residents stable and out of the hospital.
Remote Patient Monitoring reduces SNF hospital readmissions by enabling early detection of clinical deterioration through continuous vital sign tracking. RPM data triggers clinical alerts before conditions escalate to emergency transfers, directly improving the SNF Readmission Measure (SNFRM) that determines Value-Based Purchasing payment adjustments. Facilities using RPM typically see 15-30% reductions in potentially avoidable hospitalizations.
The SNF Readmission Problem
Hospital readmissions from skilled nursing facilities represent one of the most consequential quality and financial challenges in post-acute care. CMS data consistently shows that a significant share of SNF residents are rehospitalized within 30 days of admission — with conditions like heart failure, pneumonia, COPD exacerbation, and urinary tract infections driving the majority of potentially avoidable transfers.
The SNF Value-Based Purchasing Program
The SNF Value-Based Purchasing (VBP) program, established by the Protecting Access to Medicare Act of 2014 and implemented by CMS beginning in FY 2019, ties Medicare Part A payments directly to readmission performance. The program's mechanics are straightforward but consequential:
- CMS withholds 2% of each SNF's Medicare Part A payments and places them into a shared incentive pool
- Facilities are scored on the SNF 30-Day All-Cause Readmission Measure (SNFRM) — which tracks hospital readmissions within 30 days of SNF admission
- Performance is evaluated against both the facility's own baseline (improvement scoring) and national benchmarks (achievement scoring) — the higher of the two scores determines the payment adjustment
- High-performing facilities earn back more than the 2% withhold; low performers receive less — potentially losing a meaningful portion of their Medicare revenue
The financial impact is not theoretical. The 2% withhold applies to the entirety of a facility's Medicare Part A claims, which for many SNFs represents millions of dollars annually. Even a partial loss of the incentive redistribution translates to tens of thousands of dollars in reduced revenue per year.
Why Readmissions Happen
The clinical drivers of SNF readmissions are well-documented. Post-acute residents arrive at the facility in a clinically unstable state — recovering from acute illness, surgery, or cardiac events. The first 7-14 days carry the highest risk as residents stabilize on new medication regimens, adjust to care transitions, and recover baseline functional status.
The most common causes of potentially avoidable readmissions include:
- Heart failure decompensation — fluid retention, rising blood pressure, respiratory distress
- Respiratory decline — pneumonia progression, COPD exacerbation, oxygen desaturation
- Medication-related complications — adverse drug reactions, therapeutic failures, dosing errors during transitions
- Infection escalation — UTIs, skin infections, and surgical site complications that progress without early intervention
- Diabetic emergencies — hypoglycemia, hyperglycemia, and ketoacidosis from destabilized glucose management
In each of these scenarios, the clinical deterioration is gradual — developing over hours or days before reaching the threshold where emergency transfer becomes unavoidable. This is the window where RPM intervention changes outcomes.
How RPM Addresses Readmission Risk
Remote Patient Monitoring provides a systematic clinical capability that traditional manual vital sign checks cannot replicate: continuous or high-frequency physiologic data collection with automated threshold-based alerting. This is the mechanism that converts a preventable readmission into an in-facility clinical intervention.
The Early Detection Mechanism
Traditional vital sign monitoring in SNFs occurs during scheduled nursing rounds — typically every 4-8 hours depending on acuity level and staffing. Between rounds, clinical deterioration can progress undetected. A blood pressure reading at 6:00 AM might be within normal limits while the resident's pressure climbs to dangerous levels by early afternoon, with no measurement taken until the evening round.
RPM eliminates this gap. Monitoring devices capture vital signs at defined intervals (or continuously, in the case of contactless devices), and the data transmits automatically to the clinical platform. When readings cross established thresholds — a systolic blood pressure exceeding 160 mmHg, oxygen saturation dropping below 92%, or weight increasing by more than 2 pounds overnight — the system generates clinical alerts that reach the care team immediately.
Vital Sign Monitoring Protocols for Readmission Prevention
The most effective SNF RPM programs align monitoring protocols with the specific readmission risk factors for each resident:
| Condition Risk | Primary Vital Signs | Alert Triggers |
|---|---|---|
| Heart failure | Weight, blood pressure, SpO2, respiratory rate | Weight gain >2 lbs/day, BP >160/100, SpO2 <92% |
| COPD / Pneumonia | SpO2, respiratory rate, heart rate, temperature | SpO2 <90%, RR >24, HR >110, temp >101.5°F |
| Diabetes | Blood glucose, weight, blood pressure | Glucose <70 or >300, rapid weight change |
| Hypertension / Stroke risk | Blood pressure, heart rate | SBP >180 or <90, irregular HR patterns |
| Post-surgical | Temperature, heart rate, blood pressure, SpO2 | Temp >101°F, HR >100, BP deviation from baseline |
This condition-specific approach ensures that the monitoring intensity matches the clinical risk — capturing the specific physiologic signals that precede the readmission events most common for each resident's diagnosis profile.
The 30-Day Post-Discharge Window
The 30-day period following hospital discharge is the single highest-risk window for readmission, and it is the specific timeframe that the SNFRM measures. Understanding the risk dynamics within this window is essential for designing effective RPM protocols.
Risk Distribution Within the Window
Readmission risk is not evenly distributed across the 30-day period. The first 7 days carry disproportionate risk — this is when medication regimen changes are most likely to cause adverse effects, when clinical instability from the acute episode is highest, and when care transition failures (missed orders, incomplete handoffs, delayed therapy initiation) are most likely to manifest.
Days 8-14 represent a secondary risk peak, particularly for residents with heart failure (where fluid overload may build gradually) and respiratory conditions (where infections may progress despite initial antibiotic therapy).
RPM monitoring intensity should mirror this risk curve — with higher-frequency readings and tighter alert thresholds during the first two weeks, potentially relaxing to maintenance-level monitoring for the final two weeks as the resident stabilizes.
Care Transition Monitoring
RPM also supports the discharge transition from SNF to home or a lower level of care. When a resident leaves the SNF, the 30-day readmission clock continues running. Sending a resident home with an RPM device — a cellular blood pressure monitor, weight scale, or pulse oximeter — extends clinical oversight beyond facility walls and provides the SNF care team with visibility into the resident's condition during the vulnerable post-discharge days.
This is particularly valuable for residents discharging with chronic conditions that require ongoing management: a heart failure patient going home with a weight scale and blood pressure monitor allows the clinical team to detect early signs of decompensation and coordinate with the primary care physician before a readmission event occurs.
RPM and SNF Quality Measures
Value-Based Purchasing Performance
The most direct connection between RPM and SNF financial performance is through the VBP program. Every readmission prevented improves the facility's SNFRM score, which directly determines the VBP payment adjustment. For facilities currently receiving payment reductions — which represents the majority of SNFs — even a modest improvement in readmission rates can shift performance from a net loss to a net gain on the 2% withhold.
The financial math is compelling: a 100-bed facility with $5 million in annual Medicare Part A revenue has $100,000 at stake in the VBP program (2% of $5M). Moving from the 40th percentile to the 60th percentile on SNFRM performance could represent the difference between losing $30,000 and gaining $20,000 — a $50,000 swing from a relatively modest readmission improvement.
Five-Star Quality Rating System
While the Five-Star system uses different quality measures than VBP, RPM generates downstream improvements that affect star ratings:
- Quality Measure (QM) domain: Reduced hospitalizations improve several QM scores, including measures related to acute care utilization
- Staffing domain: RPM enables more efficient clinical resource allocation by directing nursing attention to residents with active alerts rather than uniform scheduled rounds
- Health Inspection domain: RPM-generated clinical documentation demonstrates proactive monitoring practices during survey and inspection events
QAPI Integration
RPM data feeds directly into Quality Assurance and Performance Improvement (QAPI) programs. The continuous data stream provides objective evidence for root cause analysis of adverse events, tracking of quality improvement interventions, and measurement of outcomes over time. When surveyors ask about a facility's approach to readmission prevention, RPM monitoring data and clinical alert response documentation provide concrete, auditable evidence of systematic quality improvement.
Contactless Monitoring for High-Risk Populations
Cognitively impaired SNF residents represent the highest-risk population for readmission — and the hardest to monitor with traditional RPM devices. Residents with dementia, delirium, or post-surgical cognitive changes cannot reliably operate blood pressure cuffs, step on weight scales, or clip on pulse oximeters without staff assistance.
Radar-Based Vital Sign Monitoring
Contactless monitoring devices use radar technology to measure heart rate, respiratory rate, and movement patterns without any resident interaction. The device mounts on a wall or sits on a bedside table and operates continuously — 24 hours a day, 7 days a week — capturing vital signs passively.
For readmission prevention in cognitively impaired populations, contactless monitoring provides:
- Respiratory rate trending — a rising respiratory rate is one of the earliest indicators of infection, heart failure decompensation, and COPD exacerbation. Detecting a respiratory rate increase from 16 to 22 breaths per minute over 48 hours triggers clinical assessment before the resident becomes acutely symptomatic
- Heart rate variability — changes in resting heart rate patterns can indicate developing infection, medication effects, or cardiac rhythm disturbances
- Overnight monitoring — continuous data capture during night hours, when staffing is lowest and clinical deterioration often progresses undetected
- Passive fall detection — detecting falls without wearable pendants that cognitively impaired residents may remove or refuse to wear
Bridging the Compliance Gap
From a billing perspective, contactless monitoring solves the device compliance challenge that undermines traditional RPM programs in SNF settings. CPT 99454 requires 16 days of transmitted data per 30-day billing period. When cognitively impaired residents cannot or will not operate traditional devices, reading compliance drops below the billing threshold. Contactless devices achieve near-100% compliance automatically — the resident does not need to do anything.
Implementation Considerations
Which Residents to Monitor First
A phased enrollment approach yields the best results. Start with the highest-impact, lowest-complexity residents:
Phase 1: Post-acute admissions (Weeks 1-2) Residents admitted directly from hospital discharge carry the highest readmission risk and generate the clearest ROI. Enroll all post-acute admissions in RPM monitoring with condition-specific vital sign protocols upon arrival.
Phase 2: Chronic condition residents (Weeks 3-4) Residents with heart failure, COPD, diabetes, and hypertension who have been at the facility longer but carry ongoing readmission risk. These residents benefit from sustained monitoring and represent the largest long-term revenue opportunity.
Phase 3: Facility-wide deployment (Month 2+) Expand contactless monitoring to all residents for baseline vital sign coverage, overnight monitoring, and fall detection. This phase generates the broadest quality improvement data and the most consistent billing revenue.
Staff Training and Workflow Integration
RPM adoption in SNFs succeeds or fails based on nursing staff engagement. The platform must integrate into existing workflows — not create parallel ones. Key training elements include:
- Alert response protocols — clear escalation pathways from initial alert to clinical assessment to physician notification
- Dashboard review during shift handoffs — incorporating RPM trend data into shift change reports
- Documentation practices — ensuring clinical actions taken in response to alerts are recorded for both quality and billing purposes
- Device troubleshooting — basic device management for battery replacement, connectivity issues, and resident questions
CCN Health's Approach to Readmission Prevention
CCN Health's platform is built for the specific challenges of SNF-based readmission prevention — not adapted from a physician practice model.
Multi-Vital Monitoring With Clinical Context
The platform supports simultaneous monitoring of blood pressure, weight, pulse oximetry, glucose, heart rate, respiratory rate, temperature, and sleep patterns. Critically, these data streams are correlated — the clinical dashboard presents a unified view of each resident's physiologic status rather than isolated vital sign readings. A weight gain combined with increasing respiratory rate and blood pressure creates a different clinical picture than any single reading alone.
Clinical Alert Protocols
CCN Health's alert engine goes beyond simple threshold crossing. Alerts are configured per-resident based on diagnosis, medication profile, and individual baseline values. Trend-based alerts detect gradual deterioration patterns that single-reading thresholds would miss — the slow upward drift in weight over five days that signals heart failure decompensation before any single reading triggers an alarm.
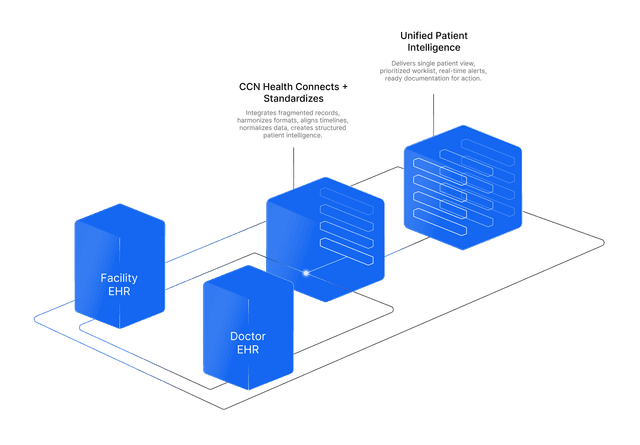
Dual-EHR Integration for SNFs
In skilled nursing, monitoring data must reach both the facility EHR (PointClickCare, ALIS, MatrixCare, or August Health) and the attending physician's EHR (athenahealth, Epic, or another practice system). CCN Health's dual-EHR architecture bridges both systems simultaneously — ensuring nursing staff see alert data in PCC and physicians receive clinical summaries in their own system. This eliminates the communication gaps that contribute to delayed intervention and preventable readmissions.
RPM + CCM Program Stacking
The most effective readmission prevention combines RPM monitoring with CCM care coordination. RPM captures the physiologic data; CCM provides the structured clinical follow-up — medication reconciliation, care plan adherence, specialist coordination, and patient education. CCN Health supports both programs on a single platform, enabling facilities to address the two primary drivers of preventable readmissions (undetected clinical deterioration and inadequate care coordination) within one integrated workflow.
For qualifying residents, stacking RPM (CPT 99453-99458) with CCM (CPT 99490-99491) generates direct reimbursement of approximately $165-$240 per resident per month — making readmission prevention not just a quality initiative but a revenue-generating clinical program.
The Path Forward
The SNF VBP program is not going away. CMS has consistently expanded value-based payment models across post-acute care settings, and readmission performance will only become more consequential to facility financial viability. Facilities that invest in systematic readmission prevention now — through continuous monitoring, early intervention protocols, and structured care coordination — will be positioned to earn incentive payments rather than absorb penalties.
RPM provides the clinical infrastructure to make that shift. It transforms readmission prevention from a reactive effort (identifying problems after they become emergencies) into a proactive clinical capability (detecting deterioration before it becomes irreversible). Combined with CCM care coordination and contactless monitoring for high-risk populations, RPM gives SNF clinical teams the tools to keep residents stable, out of the hospital, and on track with their recovery plans.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. VBP payment adjustments and readmission rate impacts are estimates based on CMS program documentation and industry benchmarks — actual results will vary by facility. Always consult qualified healthcare, billing, and regulatory professionals for guidance specific to your facility.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Early Clinical Intervention
Continuous vital sign monitoring detects deterioration hours or days before it becomes an emergency — giving clinical staff time to intervene and prevent hospital transfers.
VBP Payment Protection
Improved readmission rates translate directly to higher VBP incentive payments and avoided Medicare payment reductions — protecting your facility's financial performance.
Objective Clinical Documentation
RPM generates timestamped, device-verified clinical data that supports medical decision-making and provides audit-ready documentation of monitoring and intervention.
Post-Discharge Monitoring
Extend clinical oversight through the critical 30-day post-discharge window — monitoring residents during care transitions when readmission risk is highest.
Contactless Monitoring Options
Radar-based contactless devices monitor vital signs for memory care and cognitively impaired residents who cannot use traditional RPM devices or self-report symptoms.
Multi-Program Revenue
RPM generates direct reimbursement through CPT 99453-99458 while simultaneously improving quality metrics — creating both a revenue stream and cost avoidance.
Continue Reading
Related Articles
Explore more insights on this topic.
Best RPM Solutions for Skilled Nursing Facilities in 2026
A guide to the best RPM solutions purpose-built for skilled nursing facilities — covering PointClickCare integration, dual-EHR data flow, contactless monitoring for cognitively impaired residents, and Medicare billing optimization for post-acute and long-term care.
PDPM and RPM: How Remote Monitoring Supports SNF Reimbursement Optimization
RPM data strengthens PDPM classification accuracy in skilled nursing facilities — supporting NTA and Nursing component scoring, improving clinical documentation, and generating separate Medicare revenue alongside the per-diem payment model.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
The SNF VBP program, established by the Protecting Access to Medicare Act of 2014, adjusts Medicare Part A payments to skilled nursing facilities based on their performance on the SNF 30-Day All-Cause Readmission Measure (SNFRM). CMS withholds 2% of SNF Medicare payments and redistributes them based on each facility's readmission performance relative to their own baseline and national benchmarks. Facilities with lower readmission rates receive incentive payments, while those with higher rates lose a portion of their Medicare revenue.
RPM provides continuous or scheduled monitoring of vital signs — blood pressure, heart rate, oxygen saturation, weight, and glucose — for SNF residents. When readings fall outside established thresholds, the system generates clinical alerts that prompt nursing staff to intervene early. For example, a gradual increase in weight combined with decreasing oxygen saturation might indicate worsening heart failure — allowing the care team to adjust medications and avoid an emergency hospital transfer. This early intervention capability is the primary mechanism by which RPM reduces readmissions.
The most impactful vital signs for readmission prevention are blood pressure (hypertensive emergencies and stroke risk), weight (heart failure exacerbation indicator), pulse oximetry (respiratory deterioration), blood glucose (diabetic emergencies), and heart rate (cardiac arrhythmia detection). Contactless monitoring solutions add respiratory rate and sleep pattern tracking, which can detect early signs of infection or respiratory decline. The specific monitoring protocol should be tailored to each resident's discharge diagnoses and readmission risk factors.
RPM does not directly factor into the CMS Five-Star Quality Rating System, but it indirectly improves several quality measures that contribute to star ratings. By reducing hospitalizations, RPM improves the readmission-related quality measures. The clinical data generated by RPM also supports better documentation of care processes, which can improve clinical quality measure scores. Additionally, families increasingly ask about technology-enabled monitoring when selecting facilities, making RPM a competitive differentiator.
Yes. RPM is particularly valuable during the 30-day post-acute care transition period when readmission risk is highest. For residents transitioning from hospital to SNF, RPM provides continuous monitoring during the critical stabilization period. For residents discharging from SNF to home, RPM can extend clinical oversight beyond facility walls — allowing the SNF care team to monitor vital signs remotely and intervene if conditions deteriorate during the transition home.
RPM ROI for readmission prevention includes three components: avoided VBP payment reductions (up to 2% of Medicare Part A revenue), direct RPM reimbursement through CPT codes 99453-99458 (approximately $103-141 per patient per month), and avoided costs of emergency hospital transfers. For a typical 100-bed SNF, even a modest readmission reduction can translate to significant savings — particularly when combined with the direct RPM revenue stream. The monitoring technology cost is typically far outweighed by these combined financial benefits.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.