Guides
PDPM and RPM: How Remote Monitoring Supports SNF Reimbursement Optimization
RPM data strengthens PDPM classification accuracy in skilled nursing facilities — supporting NTA and Nursing component scoring, improving clinical documentation, and generating separate Medicare revenue alongside the per-diem payment model.
Remote Patient Monitoring supports PDPM reimbursement in skilled nursing facilities by providing objective, continuous clinical data that strengthens classification accuracy across the Nursing and Non-Therapy Ancillary (NTA) components. RPM vital sign data documents clinical complexity for higher Nursing case-mix groups, supports comorbidity capture for NTA scoring, and generates separate Medicare revenue through CPT 99453-99458 — complementing rather than overlapping with the PDPM per-diem payment.
Understanding PDPM: The SNF Payment Model
The Patient-Driven Payment Model (PDPM) replaced the Resource Utilization Group (RUG-IV) system on October 1, 2019, fundamentally changing how Medicare reimburses skilled nursing facilities for Part A stays. Under RUG-IV, reimbursement was heavily tied to therapy minutes — creating a perverse incentive to maximize therapy volume rather than deliver clinically appropriate care.
PDPM shifted to a patient-characteristics model. Each resident's per-diem payment is now determined by five independently scored case-mix adjustment components:
- Physical Therapy (PT) — based on functional status and clinical category
- Occupational Therapy (OT) — based on functional status and clinical category
- Speech-Language Pathology (SLP) — based on cognitive status, swallowing disorders, and clinical category
- Nursing — based on clinical complexity, conditions, and services documented on the MDS
- Non-Therapy Ancillary (NTA) — based on comorbidity burden, extensive services, and certain clinical conditions
Each component has its own case-mix group, its own base rate, and its own classification methodology. The Nursing and NTA components together account for approximately 43% of the total PDPM per-diem payment — and these are the two components where RPM data has the most direct impact on classification accuracy.
Where RPM Data Strengthens PDPM Classification
RPM does not change PDPM classification rules. It provides better clinical data to apply those rules accurately.
The gap in many SNFs is not intentional under-coding — it is incomplete clinical documentation. When vital signs are captured intermittently (once or twice per shift during manual rounds), the clinical record may not fully reflect a resident's condition complexity. RPM closes that documentation gap with continuous, objective, time-stamped physiologic data.
The Nursing Component
The PDPM Nursing component assigns residents to case-mix groups based on clinical conditions and services documented in the Minimum Data Set (MDS) assessment. Higher Nursing case-mix groups correspond to greater clinical complexity — and higher per-diem reimbursement.
Clinical conditions that drive Nursing component classification include:
- Cardiovascular instability — labile blood pressure, heart rate irregularities, fluid retention
- Respiratory compromise — oxygen dependency, desaturation events, abnormal respiratory patterns
- Metabolic complexity — glucose instability, weight fluctuations, electrolyte-related symptoms
- Post-surgical monitoring needs — vitals trending during recovery, wound-related complications
RPM devices capture these clinical signals continuously. A cellular blood pressure monitor documents daily readings that reveal patterns — labile hypertension, orthostatic changes, medication response — that two manual readings per day cannot capture. A pulse oximeter worn during sleep identifies nocturnal desaturation events that occur between nursing rounds. A weight scale detects the 2-3 pound daily fluctuations that signal early heart failure decompensation.
This data does not inflate clinical complexity. It documents complexity that already exists but may be missed by intermittent manual assessment. When the MDS coordinator completes the assessment, the clinical record contains objective evidence supporting accurate condition coding — which in turn supports accurate Nursing component classification.
The NTA Component
The Non-Therapy Ancillary component reimburses SNFs for the cost of non-therapy services — medications, medical supplies, lab work, and clinical monitoring. NTA scoring is driven primarily by comorbidity burden: the more qualifying comorbid conditions a resident has, and the more clinically complex those conditions are, the higher the NTA case-mix group.
NTA classification uses ICD-10 diagnosis codes and MDS items to identify qualifying conditions. Common conditions that affect NTA scoring include:
- Heart failure (ICD-10: I50.x) — supported by daily weight monitoring, blood pressure trending
- COPD and respiratory conditions (ICD-10: J44.x) — supported by SpO2 monitoring, respiratory rate tracking
- Diabetes with complications (ICD-10: E11.x) — supported by glucose monitoring, CGM data
- Hypertensive disease (ICD-10: I10-I15) — supported by continuous blood pressure data
- Chronic kidney disease (ICD-10: N18.x) — supported by weight and fluid balance monitoring
RPM data supports NTA scoring by documenting the active clinical management of these comorbid conditions. When a resident has diabetes documented on the MDS, supporting that diagnosis with continuous glucose monitoring data demonstrates ongoing clinical activity that validates the comorbidity coding. This is especially important during audits, where documentation of active condition management strengthens the clinical justification for NTA classification.
RPM as a Complementary Revenue Stream
One of the most important distinctions for SNF administrators: RPM does not compete with PDPM. It complements it.
PDPM covers Medicare Part A skilled nursing services — the per-diem rate for residents in a covered SNF stay. RPM is billed separately under Medicare Part B through its own CPT code family:
| CPT Code | Description | Reimbursement (est.) |
|---|---|---|
| 99453 | Initial device setup and patient education | ~$22 (one-time) |
| 99454 | Device supply with daily recording/transmission (16+ days/month) | ~$52/month |
| 99457 | First 20 minutes of RPM clinical monitoring time | ~$52/month |
| 99458 | Each additional 20 minutes of clinical monitoring time | ~$41/month |
A single resident generating CPT 99454 + 99457 + 99458 produces approximately $104–$186 per month in Part B RPM revenue. This revenue is entirely separate from the PDPM per-diem payment — different CPT codes, different Medicare part, different billing entity (the physician bills RPM under Part B, while the facility receives PDPM under Part A).
For a 100-bed SNF with 50 residents enrolled in RPM, this represents $62,400–$111,600 in annual revenue that sits completely outside the PDPM payment structure.
Stacking Beyond RPM
Qualifying residents can also receive CCM (Chronic Care Management, CPT 99490-99491), PCM (Principal Care Management, CPT 99424-99427), BHI (Behavioral Health Integration, CPT 99484), and RTM (Remote Therapeutic Monitoring, CPT 98975-98981) — all billed under Part B alongside the Part A PDPM payment. A resident with multiple qualifying conditions can generate $200-$350 per month in combined Part B program revenue, layered on top of the PDPM per-diem rate.
RPM's Impact on Discharge Planning and Quality Measures
PDPM includes a variable per-diem adjustment that decreases payment over time during a SNF stay, creating a financial incentive for appropriate discharge timing. Accurate discharge planning requires reliable clinical data — and this is another area where RPM contributes.
Data-Driven Discharge Decisions
Continuous vital sign trending provides the clinical evidence to support discharge readiness. Rather than relying on snapshot assessments, clinicians can review multi-day trends:
- Blood pressure stability — a resident whose daily readings show consistent control is clinically ready for a lower-acuity setting
- Weight stability — no significant fluctuation over 5-7 days indicates resolved fluid retention
- SpO2 consistency — sustained adequate oxygenation without supplementation supports discharge
- Heart rate and respiratory rate patterns — stable baselines confirm clinical improvement
This objective data supports the clinical decision to discharge, reduces premature discharges that lead to readmission, and provides documentation that justifies the length of stay if questioned during an audit.
The SNF Value-Based Purchasing Connection
The SNF Value-Based Purchasing (VBP) Program adjusts Medicare payments based on 30-day all-cause hospital readmission rates. Facilities with lower readmission rates receive payment incentives; facilities with higher rates face payment reductions of up to 2%.
RPM directly supports readmission reduction through:
- Early deterioration detection — vital sign changes are identified hours or days before they would be caught during scheduled nursing rounds
- Post-discharge monitoring continuity — residents transitioning from SNF to home or assisted living can continue RPM monitoring, maintaining clinical visibility during the critical 30-day window
- Clinical intervention triggers — automated alerts notify clinical staff when readings breach established thresholds, enabling timely intervention before deterioration becomes an emergency
A 100-bed facility avoiding even three to four readmissions per year through RPM monitoring can see meaningful improvement in its VBP score — protecting existing Medicare payment rates and potentially earning incentive payments.
How CCN Health Supports PDPM-Aware SNF Monitoring
CCN Health is purpose-built for the skilled nursing environment where PDPM documentation and RPM data collection intersect. Several platform capabilities are specifically relevant for SNFs managing both revenue streams.
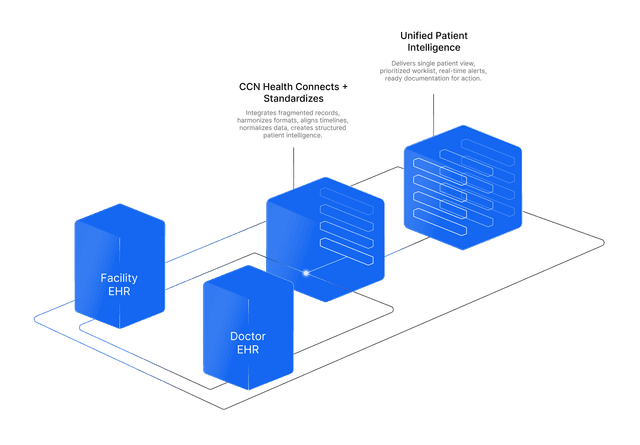
Dual-EHR Data Flow
In most SNFs, the facility uses PointClickCare for resident care documentation (including MDS assessments that drive PDPM classification) while attending physicians use a separate EHR for clinical orders and Part B billing (including RPM).
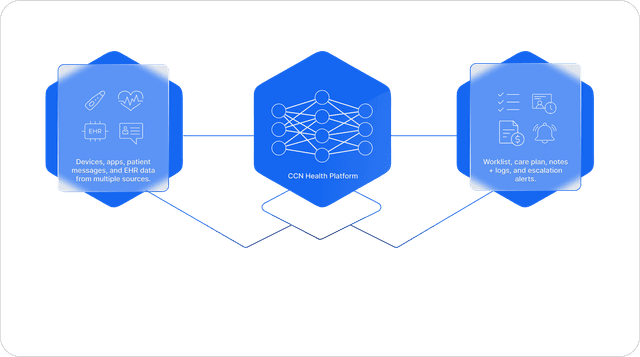
CCN Health bridges both systems simultaneously:
- RPM vital sign data flows to PointClickCare — ensuring the clinical record available to the MDS coordinator includes continuous monitoring data that supports accurate PDPM classification
- The same data flows to the physician's EHR (athenahealth, Epic, or another system) — supporting the clinical documentation required for Part B RPM billing
- No manual data transcription between systems — eliminating the documentation gaps that lead to under-classification on MDS assessments or incomplete RPM billing records
Automated Clinical Documentation
Every vital sign reading, threshold alert, and clinical response is documented automatically in the resident's record. This documentation serves dual purposes:
- PDPM support — provides the clinical evidence of condition complexity that MDS coordinators reference during assessments
- RPM billing support — documents the device data transmission and clinical monitoring time required for CPT code compliance
Contactless Monitoring for Cognitively Impaired Residents
Many SNF residents under PDPM have cognitive impairments that prevent reliable use of traditional RPM devices. CCN Health supports the Xandar Kardian XK300 — a radar-based contactless monitor that captures heart rate, respiratory rate, and fall events without any resident interaction. These residents receive continuous monitoring that supports both PDPM clinical documentation and RPM billing compliance at near-100% data collection rates.
Device Flexibility Across Clinical Conditions
Different PDPM clinical categories require different monitoring approaches. CCN Health supports 25+ FDA-cleared devices across the full spectrum of conditions seen in SNFs:
- Blood pressure monitors — for cardiovascular conditions (Nursing and NTA component relevance)
- Weight scales — for heart failure, CKD, and fluid management
- Pulse oximeters — for respiratory conditions and post-acute recovery
- Glucose monitors and CGMs — for diabetes with complications
- Contactless monitors — for cognitively impaired residents across all clinical categories
This device flexibility means the monitoring program adapts to each resident's clinical profile rather than applying a one-size-fits-all approach — resulting in data that more accurately reflects the clinical complexity relevant to PDPM classification.
Implementation: Adding RPM to a PDPM-Focused SNF
For SNFs already optimizing PDPM classification, adding RPM is operationally straightforward when the platform integrates with existing EHR infrastructure.
Phase 1: Identify High-Value Residents
Start with residents who have documented comorbid conditions that are both PDPM-relevant and RPM-appropriate — hypertension, heart failure, COPD, diabetes. These residents generate the strongest clinical documentation overlap: the RPM data strengthens their PDPM classification while simultaneously generating Part B revenue.
Phase 2: Deploy Devices and Integrate Data
CCN Health handles device deployment, cellular connectivity, and EHR integration. Vital sign data begins flowing to the facility EHR immediately — the MDS coordinator gains access to continuous clinical data for the next scheduled assessment without any workflow change.
Phase 3: Expand Enrollment
Once the initial cohort demonstrates both documentation improvement and revenue generation, expand enrollment to additional residents — including those receiving post-acute care, residents with behavioral health needs (BHI opportunity), and cognitively impaired residents using contactless monitoring.
The Bottom Line
PDPM and RPM are not competing payment models — they are complementary systems that, when properly integrated, strengthen both clinical documentation and financial performance for skilled nursing facilities. PDPM pays the facility a per-diem rate based on clinical classification. RPM generates separate Part B revenue while providing the continuous clinical data that supports accurate classification under the Nursing and NTA components.
For SNFs already investing in PDPM optimization, RPM is the natural next step: better data for classification, better documentation for audits, better clinical visibility for discharge planning, and a new revenue stream that sits entirely outside the Part A per-diem structure.
This article is for informational purposes only and does not constitute billing, coding, or legal advice. PDPM classification decisions should be made by qualified MDS coordinators based on CMS guidelines. RPM billing and coding should be reviewed by qualified compliance professionals. Medicare reimbursement rates are approximate and subject to annual fee schedule updates. Facilities should consult with their compliance and billing teams before implementing any changes to their reimbursement strategy.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Stronger PDPM Classification
Continuous RPM data provides objective clinical evidence that supports accurate Nursing and NTA component scoring — reducing the risk of under-classification on MDS assessments.
Complementary Revenue Stream
RPM generates $104-186 per resident per month through Part B CPT codes, layering on top of PDPM per-diem payments without billing conflict or overlap.
Clinical Documentation Depth
Automated vital sign trending and alert documentation flows directly into the facility EHR, strengthening the clinical record that supports PDPM classification decisions.
Readmission Reduction
Continuous monitoring during the post-acute window detects clinical deterioration early — protecting SNF VBP scores and future Medicare reimbursement rates.
Comorbidity Capture
Ongoing RPM data for chronic conditions supports accurate ICD-10 coding and MDS documentation, ensuring NTA component scoring reflects true comorbidity burden.
Dual-EHR Integration
CCN Health bridges the facility EHR (for PDPM documentation) and physician EHR (for RPM billing) simultaneously — eliminating manual data transcription between systems.
Continue Reading
Related Articles
Explore more insights on this topic.
Best RPM Solutions for Skilled Nursing Facilities in 2026
A guide to the best RPM solutions purpose-built for skilled nursing facilities — covering PointClickCare integration, dual-EHR data flow, contactless monitoring for cognitively impaired residents, and Medicare billing optimization for post-acute and long-term care.
How RPM Reduces SNF Readmissions and Avoids VBP Penalties
73% of skilled nursing facilities face Value-Based Purchasing payment adjustments tied to hospital readmission rates. RPM provides early clinical intervention that keeps residents stable and out of the hospital.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
No. PDPM is a per-diem payment model covering Part A skilled nursing services, while RPM is billed separately under Medicare Part B through CPT codes 99453-99458. The two payment streams are distinct — PDPM covers the facility's daily rate based on clinical classification, and RPM reimburses for physiologic monitoring services ordered by a physician. There is no overlap or double-billing concern when both are properly documented and billed through the appropriate Medicare parts.
The PDPM Nursing component classifies residents based on clinical complexity indicators documented in the MDS assessment. Continuous RPM data — blood pressure trends, oxygen saturation patterns, weight fluctuations, heart rate variability — provides objective evidence of clinical conditions that drive higher Nursing case-mix groups. For example, a resident with documented labile hypertension (supported by daily blood pressure readings from RPM) is more accurately classified than one relying solely on intermittent manual vitals.
The Non-Therapy Ancillary (NTA) component reimburses SNFs for non-therapy services based on the resident's comorbidity burden and certain clinical indicators. NTA scoring uses ICD-10 codes and MDS items to assign a case-mix group. RPM data supports NTA scoring by documenting the active management of comorbid conditions — continuous glucose monitoring for diabetes, weight trending for heart failure, SpO2 tracking for COPD — providing clinical evidence that justifies the comorbidity coding used in NTA classification.
Yes. SNFs can bill RPM for residents concurrently receiving PDPM-covered services, provided the RPM is ordered by a physician and billed under Part B. The RPM must use FDA-cleared devices, transmit data for at least 16 days per month, and include qualifying clinical monitoring time (CPT 99457-99458). Many SNF residents — particularly those with chronic conditions like hypertension, diabetes, COPD, and heart failure — qualify for both PDPM skilled services and ongoing RPM monitoring.
The SNF Value-Based Purchasing (VBP) Program adjusts Medicare payments based on 30-day hospital readmission rates. RPM directly supports readmission reduction by providing continuous clinical monitoring during the high-risk post-acute period. Early detection of vital sign changes — rising blood pressure, weight gain indicating fluid retention, declining SpO2 — enables clinical intervention before deterioration requires rehospitalization. Lower readmission rates improve the facility's VBP score, protecting and potentially increasing future Medicare payments.
The most relevant RPM devices for SNF residents under PDPM include cellular blood pressure monitors (for hypertension and cardiac conditions), weight scales (for heart failure and fluid retention monitoring), pulse oximeters (for respiratory conditions like COPD and pneumonia recovery), glucose monitors and CGMs (for diabetes management), and contactless monitors like the Xandar Kardian XK300 (for continuous heart rate, respiratory rate, and fall detection in cognitively impaired residents). All devices should use cellular connectivity for reliability in facility environments.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.