market-news
How RPM Reimbursement Is Changing in 2026: CMS Updates and Revenue Impact
CMS has made several adjustments to RPM reimbursement for 2026 — from updated fee schedule rates to expanded device eligibility and refined documentation requirements. Here's what providers need to know to protect and maximize RPM revenue.
RPM reimbursement in 2026 reflects major CMS updates including two new CPT codes (99445 and 99470), rate increases across all codes, and refined documentation requirements. The 2026 rates: 99453 device setup (~$22 one-time), 99454 device supply 16+ days (~$52/mo), 99445 device supply 2–15 days (~$52/mo, new), 99457 first 20 min management (~$52/mo), 99470 first 10 min management (~$26/mo, new), 99458 additional 20 min (~$41/mo). Total per-patient monthly revenue ranges from approximately $78 (new lower-threshold codes) to $245+ depending on engagement and services rendered.
The RPM Reimbursement Landscape in 2026
The CY 2026 Medicare Physician Fee Schedule (PFS) final rule, published by CMS in November 2025, delivered the most significant structural update to RPM billing since the code family was introduced. While prior years focused on rate preservation and incremental adjustments, the 2026 rule expands the RPM billing framework itself — adding two new CPT codes, lowering monitoring thresholds, and increasing reimbursement rates across the board.
For providers already operating RPM programs, these changes mean higher per-patient revenue potential and the ability to bill for patients who previously fell outside the 16-day data transmission window. For organizations evaluating whether to launch RPM, the 2026 rule removes several barriers that historically limited enrollment and made the financial case harder to prove for smaller patient populations.
The 2026 PFS conversion factor increased to $33.40 for non-qualifying APM participants (up from $32.35 in 2025), representing a 3.26% increase. Qualifying APM participants receive a slightly higher conversion factor of $33.57. These across-the-board increases lift reimbursement for all RPM codes proportionally.
This article breaks down every change that affects RPM revenue in 2026 — from updated rates and new codes to documentation expectations and program stacking strategies.
2026 RPM CPT Code Rate Table
The table below reflects the national average Medicare reimbursement rates under the 2026 PFS. Actual payment varies by geographic locality and practice setting.
| CPT Code | Description | 2025 Rate | 2026 Rate | Change | Frequency |
|---|---|---|---|---|---|
| 99453 | Initial device setup and patient education | ~$19.32 | ~$21.71 | +$2.39 | One-time per episode |
| 99445 | Device supply, 2-15 days of data transmission per 30-day period (NEW) | — | ~$52.11 | New code | Monthly |
| 99454 | Device supply, 16-30 days of data transmission per 30-day period | ~$43.02 | ~$52.11 | +$9.09 | Monthly |
| 99470 | First 10 minutes of treatment management, including interactive communication (NEW) | — | ~$26.05 | New code | Monthly |
| 99457 | First 20 minutes of treatment management, including interactive communication | ~$47.87 | ~$51.77 | +$3.90 | Monthly |
| 99458 | Each additional 20 minutes of treatment management | ~$38.19 | ~$41.42 | +$3.23 | Monthly (up to 2x) |
| 99091 | Collection and interpretation of physiologic data, 30+ minutes | ~$55.78 | ~$58.48 | +$2.70 | Monthly |
Key billing rules for the new codes:
- 99445 and 99454 are mutually exclusive. Bill one or the other per 30-day period based on the actual number of data transmission days. If a patient transmits data for 16 or more days, bill 99454. If 2 to 15 days, bill 99445.
- 99470 and 99457 are mutually exclusive. Bill based on total treatment management time in the calendar month. If clinical staff spend 10 to 19 minutes, bill 99470. At 20 minutes or more, bill 99457 (and add 99458 for each additional 20-minute increment).
- 99091 remains separately billable for physician or qualified healthcare professional time spent interpreting physiologic data, provided the time is distinct from the treatment management time billed under 99457/99458/99470.
Revenue Scenarios Per Patient Per Month
For a single patient enrolled in RPM only:
| Scenario | Codes Billed | Estimated Monthly Revenue |
|---|---|---|
| Minimum engagement (2-15 days data, 10 min management) | 99445 + 99470 | ~$78 |
| Standard engagement (16+ days data, 20 min management) | 99454 + 99457 | ~$104 |
| Standard + extended management (16+ days, 40 min) | 99454 + 99457 + 99458 | ~$145 |
| Full billing (16+ days, 60 min + data interpretation) | 99454 + 99457 + 99458 x2 + 99091 | ~$245 |
| Initial month (includes setup) | 99453 + 99454 + 99457 | ~$126 |
These are estimates based on 2026 national average rates from the Medicare Physician Fee Schedule; actual reimbursement varies by locality and is set annually by CMS.
Key Policy Changes and Clarifications
New Lower-Threshold Codes Close Coverage Gaps
The introduction of CPT 99445 and 99470 is the headline change for 2026. These codes address a long-standing structural gap in RPM billing: patients who benefit clinically from remote monitoring but do not consistently meet the 16-day data transmission or 20-minute treatment management thresholds.
Before 2026, a patient who transmitted data for 14 days in a month generated zero reimbursement for the device supply component. A clinical interaction that lasted 15 minutes could not be billed at all. The new codes create a reimbursable pathway for these scenarios, expanding the eligible patient population significantly.
This is particularly relevant for post-surgical patients requiring short-term monitoring, patients with fluctuating engagement patterns, and senior living residents whose device interaction varies week to week.
Consent and Enrollment Requirements
The 2026 rule maintains existing consent requirements. Prior to initiating RPM services, providers must obtain and document patient consent. The patient must understand that RPM services will be furnished, that cost-sharing applies, and that only one practitioner can furnish and bill RPM services during a given service period.
CMS has not changed the requirement for an established patient relationship — meaning the billing practitioner (or a practitioner in the same billing group) must have furnished a face-to-face service to the patient within the prior year.
Supervision Requirements
General supervision continues to apply for RPM treatment management services (99457, 99458, 99470). This means clinical staff can perform these services under the overall direction of the billing practitioner without the practitioner being physically present. This framework supports scalable RPM delivery where nurses and care coordinators handle daily monitoring under physician oversight.
Device Eligibility Updates
Expanded Recognition of Contactless Monitoring
CMS has provided increasing clarity around the eligibility of contactless and ambient monitoring devices for RPM billing. Devices that passively monitor physiologic parameters — such as radar-based sensors that track heart rate, respiratory rate, and sleep patterns without requiring the patient to wear or operate anything — can qualify for RPM when they meet core requirements:
- FDA clearance as a medical device
- Digital data transmission to the ordering practitioner's practice
- Monitoring of a physiologic parameter (heart rate, respiratory rate, blood pressure, weight, blood glucose, oxygen saturation, temperature)
This expansion is particularly impactful for memory care and cognitively impaired populations, where traditional wearable devices face compliance challenges. Contactless sensors installed in a patient's room can transmit data continuously without requiring any patient interaction.
Continuous Glucose Monitors (CGMs)
CGM devices continue to qualify for RPM billing under CPT 99454 (or the new 99445 for shorter monitoring periods). The daily glucose data transmitted by devices such as the Abbott FreeStyle Libre and Dexcom G7 meets the digital data transmission requirement. The 2026 rule does not change CGM eligibility but reinforces that the data must flow to the billing practitioner's monitoring system — not just to the patient's smartphone app.
Cellular-Enabled Devices
The trend toward cellular-connected monitoring devices — blood pressure monitors, weight scales, and pulse oximeters that transmit data directly over cellular networks without requiring Wi-Fi or Bluetooth pairing — continues to simplify the data transmission requirement. These devices reduce patient setup friction and increase the likelihood of meeting the 16-day threshold for 99454 billing (or the 2-day minimum for the new 99445).
Documentation Requirements for 2026
Clinical Action, Not Just Data Collection
CMS has been increasingly clear that RPM reimbursement is predicated on clinical value — not passive data accumulation. The 2026 rule reinforces that documentation for treatment management codes (99457, 99458, 99470) must demonstrate:
- What data was reviewed — specific readings, trends, or alerts examined during the management period
- Clinical decisions made — assessment of whether vital sign trends indicate stability, improvement, or concern
- Actions taken — medication adjustments, care plan modifications, patient education delivered, referrals initiated, or escalation to the physician
- Time spent — start and stop times or total duration of clinical management activities
Practices that collect monitoring data but lack documentation showing how that data informed clinical decisions face the highest audit risk. CMS auditors increasingly look for evidence of the clinical feedback loop — data in, assessment applied, action taken.
Documentation for the New Codes
For CPT 99470 (10-19 minutes of treatment management), documentation must include evidence of at least one real-time interactive communication with the patient or caregiver during the calendar month. This interactive component differentiates treatment management from passive data review.
For CPT 99445 (2-15 days of device data), the documentation standard is the same as 99454 — the practice must show that the patient's device transmitted data on at least 2 days during the 30-day period.
Audit-Ready Documentation Checklist
Providers should ensure their RPM documentation includes:
- Patient consent documented prior to service initiation
- Ordering practitioner identified with an established patient relationship
- Device type and physiologic parameter being monitored
- Number of data transmission days per 30-day period
- Treatment management time logs with clinical narrative
- Evidence of interactive communication with patient or caregiver
- Clinical actions taken based on monitoring data
Revenue Maximization: Program Stacking in 2026
Why Single-Program RPM Leaves Revenue on the Table
RPM alone generates an estimated $104 to $245 per patient per month depending on engagement and management time. While meaningful, this represents a fraction of the revenue available when multiple Medicare care management programs are stacked for qualifying patients.
Program stacking is the practice of enrolling a single patient in multiple concurrent programs — RPM, CCM, PCM, BHI, and RTM — each billing under separate CPT code families with independently tracked clinical time. CMS permits this provided that time is not double-counted across programs.
Program Stacking Revenue Comparison
| Program Combination | Estimated Monthly Revenue | Qualifying Criteria |
|---|---|---|
| RPM only | ~$104-145 | Chronic or acute condition, FDA-cleared device |
| RPM + CCM | ~$170-211 | RPM criteria + 2 or more chronic conditions |
| RPM + CCM + BHI | ~$270-330 | Above + co-occurring behavioral health diagnosis |
| RPM + CCM + PCM | N/A — CCM and PCM are mutually exclusive | Cannot stack CCM + PCM |
| RPM + PCM | ~$175-225 | Chronic condition requiring single-disease focus |
| RPM + CCM + BHI + RTM | ~$350-450+ | Above + musculoskeletal or respiratory therapy monitoring |
| Full stack (RPM + CCM + BHI + RTM) | ~$400-500+ | All qualifying criteria met, time tracked independently |
Estimated rates based on 2026 national averages. Actual revenue varies by locality, time documented, and payer.
Optimal Patient Selection for Stacking
The highest-revenue patients are those who qualify for multiple programs simultaneously. A patient with diabetes, hypertension, depression, and chronic knee pain could qualify for RPM (blood pressure and glucose monitoring), CCM (two or more chronic conditions), BHI (co-occurring behavioral health diagnosis), and RTM (musculoskeletal therapy monitoring) — generating an estimated $400 or more per month from a single patient.
The key operational requirement is that each program's clinical time must be tracked separately and documented independently. RPM time covers device data review and clinical management. CCM time covers care coordination. BHI time covers behavioral health activities. RTM time covers therapeutic monitoring. Overlapping time is not billable.
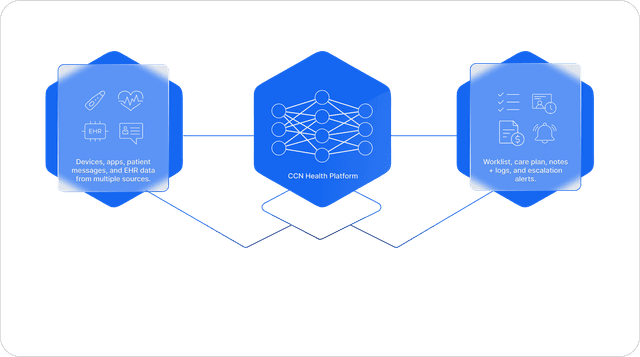
How CCN Health Helps Navigate 2026 Changes
CCN Health's platform is built around the full suite of Medicare care management programs, and the 2026 fee schedule updates align directly with capabilities the platform already supports.
Automated Data Transmission Tracking
The platform automatically counts data transmission days per patient per 30-day period, determining whether 99445 (2-15 days) or 99454 (16+ days) applies. This eliminates manual counting and ensures the correct code is billed every month.
Treatment Management Time Logging
Clinical staff time is tracked at the patient level with automatic threshold detection. The system identifies whether a patient's monthly management time qualifies for 99470 (10-19 minutes), 99457 (20+ minutes), or 99457 plus one or more units of 99458 — and generates the appropriate documentation.
Multi-Program Enrollment and Billing
CCN Health supports concurrent enrollment in RPM, CCM, PCM, BHI, and RTM with independent time tracking across programs. The platform prevents time from being double-counted and flags when a patient qualifies for additional programs based on their diagnosis profile and monitoring data.
Device-Agnostic Architecture
The platform supports 25+ FDA-cleared monitoring devices — including cellular blood pressure monitors, weight scales, pulse oximeters, continuous glucose monitors, and contactless radar sensors. This device breadth ensures providers can match the right device to each patient's clinical needs and physical capabilities, maximizing both clinical outcomes and data transmission compliance.
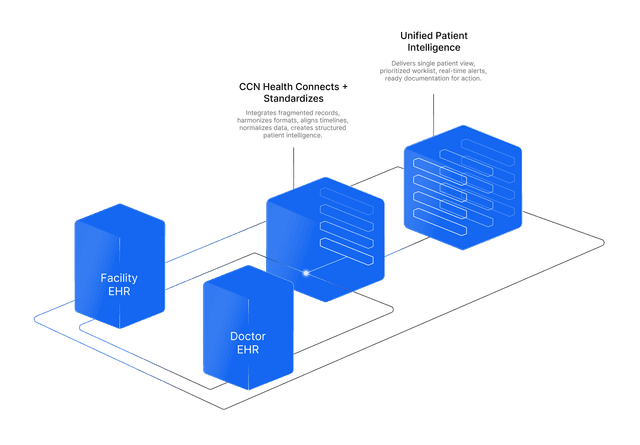
EHR Integration for Documentation Compliance
Bi-directional integrations with 8 EHR systems (including PointClickCare, ALIS, athenahealth, Epic, MatrixCare, and others) ensure that monitoring data, clinical notes, and billing documentation flow directly into the provider's existing clinical record. This integration supports the documentation standards CMS expects and reduces audit risk by maintaining a complete clinical trail in the EHR.
Looking Ahead
The 2026 PFS represents a structural expansion of RPM billing, not just a rate adjustment. The new lower-threshold codes (99445 and 99470) signal that CMS recognizes the clinical value of remote monitoring even for patients who do not meet the traditional 16-day and 20-minute thresholds. Combined with rate increases across all existing codes and the continued viability of multi-program stacking, 2026 is the strongest revenue environment for RPM that Medicare has ever offered.
Providers who act on these changes — updating their billing workflows, expanding device eligibility screening, training clinical staff on the new codes, and optimizing program stacking — will capture the full revenue potential. Those who continue billing under the old framework alone will leave the new-code revenue on the table.
This article is for informational purposes only and does not constitute legal, billing, or compliance advice. Reimbursement rates cited are estimates based on publicly available CMS fee schedule data and may vary by geographic locality, practice setting, and payer. Providers should consult with qualified billing professionals and verify current rates through the official CMS Physician Fee Schedule lookup tool before making billing decisions. CPT is a registered trademark of the American Medical Association.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
Updated Revenue Projections
2026 fee schedule rates provide clear per-patient revenue modeling — from single-program RPM to multi-program stacking strategies generating $300+ per patient monthly.
Expanded Device Eligibility
Broader CMS recognition of contactless and ambient monitoring devices creates new enrollment opportunities for populations previously excluded from RPM.
Documentation Clarity
Refined CMS documentation guidance reduces audit ambiguity — providers who demonstrate clinical action on monitoring data face lower compliance risk.
Program Stacking Revenue
RPM + CCM + PCM + BHI + RTM stacking continues as the most effective Medicare revenue strategy, with 2026 rates supporting $300-500+ per qualifying patient.
Telehealth Continuity
Continued telehealth policy support ensures the remote care infrastructure underlying RPM programs remains viable and reimbursable.
Compliance Framework
Clear 2026 rules make it easier to build compliant RPM programs — from device selection through documentation to billing submission.
Continue Reading
Related Articles
Explore more insights on this topic.
CPT Code 99091: RPM Data Collection and Interpretation Billing Guide
CPT 99091 reimburses physicians for collecting and interpreting physiologic data transmitted remotely — a distinct RPM billing code often overlooked alongside 99453-99458. This guide covers requirements, rates, and documentation.
CCM Billing Guide: CPT Codes 99490, 99491, 99439 & Requirements
A comprehensive breakdown of all CCM CPT codes — 99490, 99491, and 99439 — covering patient eligibility, consent requirements, documentation standards, complex CCM criteria, common denials, and revenue projections for chronic care management programs.
RTM Billing Guide: Remote Therapeutic Monitoring CPT Codes & Requirements
A detailed breakdown of all RTM CPT codes — 98975, 98976, 98977, 98980, and 98981 — covering the key difference from RPM, qualifying conditions like COPD rehabilitation and post-surgical recovery, self-reported data rules, and revenue projections for remote therapeutic monitoring programs.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
The 2026 Medicare RPM national non-facility rates under the Physician Fee Schedule are: CPT 99453 (setup) ~$22, CPT 99454 (device supply 16+ days) ~$52/mo, CPT 99445 (device supply 2–15 days, new 2026) ~$52/mo, CPT 99457 (first 20 min management) ~$52/mo, CPT 99470 (first 10 min management, new 2026) ~$26/mo, CPT 99458 (additional 20 min) ~$41/mo, and CPT 99091 (data interpretation 30 min) ~$58/mo. Exact rates vary by geographic locality. Monthly revenue per patient ranges from ~$78 (lower-threshold codes 99445+99470) to ~$245+ with full billing including extended management and data interpretation.
The core RPM eligibility requirements remain consistent in 2026: the patient must have a chronic condition (acute conditions may also qualify), monitoring must use an FDA-cleared medical device, and data must be digitally transmitted to the practice. CMS has provided additional clarification on eligible device categories, particularly regarding contactless monitoring technologies and continuous glucose monitors. The requirement for an established patient relationship prior to initiating RPM also continues.
Yes. RPM continues to be billable alongside CCM (Chronic Care Management), PCM (Principal Care Management), BHI (Behavioral Health Integration), and RTM (Remote Therapeutic Monitoring) in 2026. Each program uses separate CPT code families, and clinical time cannot be double-counted across programs. This program stacking approach can generate $300-500+ per patient per month for qualifying patients enrolled in multiple programs simultaneously.
CMS has emphasized that RPM documentation must demonstrate clinical value — not just data collection. Specifically, documentation should show: what monitoring data was reviewed, what clinical decisions were made based on the data, what actions were taken (medication adjustments, care plan changes, patient education), and the time spent on these clinical activities. Practices that simply collect and store data without documented clinical interpretation face increased audit risk.
RPM was never classified as a telehealth service under CMS definitions — it is a separately billable remote monitoring service. However, the broader telehealth policy environment affects RPM delivery. Congressional extensions of telehealth flexibilities support the remote care infrastructure that RPM relies on. Providers should monitor the status of permanent telehealth legislation, as it may affect related services like virtual check-ins and e-visits that complement RPM programs.
CMS has expanded clarity on contactless monitoring device eligibility under RPM. Radar-based and sensor-based devices that meet FDA clearance requirements and digitally transmit physiologic data can qualify for RPM billing. This is significant for senior living and skilled nursing environments where traditional wearable devices may not be practical for all residents, particularly those with cognitive impairment. The device must meet the standard RPM requirements: FDA clearance, digital data transmission, and monitoring of a physiologic parameter.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.