Clinical
Principal Care Management for Home Health — 2026 Guide
How PCM works in home health — specialist-level management for homebound patients with a single high-complexity condition, post-discharge optimization, and coordination with home health agencies.
PCM for home health patients provides specialist-level management of a single complex condition for homebound patients — advanced heart failure, severe COPD, or uncontrolled diabetes requiring frequent medication adjustment. PCM coordinates between the ordering specialist, home health agency, and patient/caregiver. Revenue is ~$75–115/patient/month, stacking with RPM for $250–335. PCM can continue after the home health episode ends.
What Is Principal Care Management (PCM)?
Principal Care Management (PCM) is a Medicare-reimbursable program that provides focused management of a single high-complexity chronic condition for Medicare beneficiaries, including frequent medication adjustment, specialist coordination, and disease-specific clinical oversight.
Patient eligibility: Medicare beneficiaries with a single high-complexity chronic condition requiring frequent medication adjustment or specialist management. Cannot be billed concurrently with CCM.
How PCM differs from related programs: PCM targets a single high-complexity condition (unlike CCM's 2+ conditions). It offers higher per-patient revenue than CCM and is ideal for specialist-managed conditions like uncontrolled diabetes or advanced heart failure.
PCM can be stacked with RPM, RTM for qualifying patients — a single enrolled patient can generate revenue across multiple Medicare programs simultaneously.
Why Home Health Agencies Need PCM
Home health patients with a dominant complex condition face a management gap: specialist appointments happen monthly, home health visits 1–3 times weekly, and between both, the condition is essentially unmanaged. PCM fills this gap.
Between-appointment management: Specialists see patients monthly at most — PCM provides continuous condition management between visits, coordinating medication adjustments and monitoring results
Home health nurse augmentation: HH nurses are generalists who visit episodically — PCM provides the specialist-level condition expertise that supplements their broad clinical skills
Post-discharge condition optimization: Many HH patients are post-discharge with a condition still being stabilized — PCM provides the intensive specialist coordination needed during this optimization period
Caregiver coordination: Homebound patients often rely on caregivers — PCM includes caregiver education and communication as part of the condition management strategy
How PCM Works in Home Health — The Clinical Workflow
Home health PCM bridges the specialist, home health agency, patient, and caregiver — ensuring continuous condition management at home.
Step 1: Specialist Order — Ordering specialist prescribes PCM for their homebound patient. Condition complexity assessed and PCM care plan initiated with condition-specific targets.
Step 2: Home Management Plan — Condition-specific management plan adapted for home environment — medication schedules, symptom monitoring checklist for caregiver, intervention triggers, and specialist contact protocols.
Step 3: Continuous Coordination — Monthly 30+ minute management: medication adjustment coordination, lab result follow-up, HH nurse briefings before visits, caregiver check-ins, and specialist communication.
Step 4: Beyond HH Episode — PCM continues after home health discharge — maintaining specialist management for the complex condition even when skilled visits are no longer required.
PCM Coordinates Care — RPM Monitors at Home
PCM + cellular RPM devices provide comprehensive home-based condition management — specialist coordination plus real-time vital sign monitoring.
- No devices for PCM — PCM bills for specialist management time
- Cellular RPM recommended — Bodytrace BP, weight scale, or pulse oximeter with built-in cellular — provides condition-specific data that informs PCM management at home
For home-based PCM, cellular RPM devices are the monitoring partner — no facility infrastructure, no Wi-Fi dependency, just simple cellular devices providing data for specialist management decisions.
PCM Billing: CPT Codes and Revenue
| CPT Code | Service | Reimbursement | Requirement |
|---|---|---|---|
| 99424 | PCM Services | ~$70/mo | 30+ min clinical staff time |
| 99425 | Additional 30 min | ~$47/mo | Each additional 30 min |
| 99426 | PCM (Physician) | ~$83/mo | 30+ min physician/QHP time |
| 99427 | Additional 30 min | ~$47/mo | Each additional 30 min |
Estimated monthly revenue per patient: ~$75–115
Program stacking: PCM + RPM generates $250–335/patient/month. For rehab patients, PCM + RPM + RTM can reach $350–490/month.
PCM is billed by the ordering specialist — separate from home health billing. Both can run concurrently. PCM continues after the HH episode ends, providing ongoing specialist revenue. For complex post-discharge conditions, PCM may generate more per-patient value than CCM.
EHR Integration for PCM in Home Health
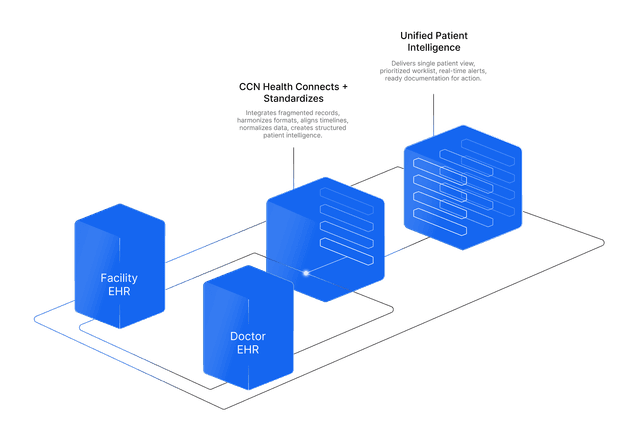
Home Health agencies typically use Practice EHRs (athenahealth, Epic, Charm Health) for clinical documentation. Home health agencies use practice EHRs rather than facility EHRs. Monitoring data routes directly to the ordering physician. No facility infrastructure to rely on.
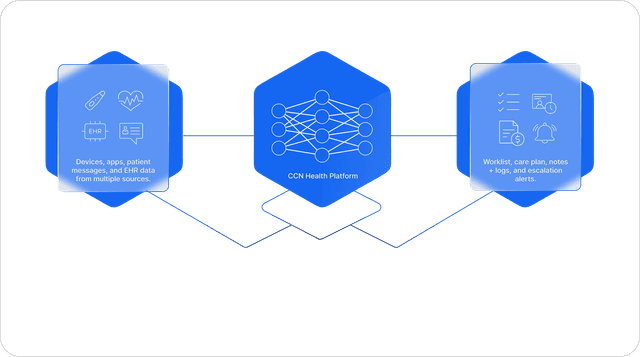
CCN Health provides bi-directional integration with all major home health EHR systems:
- Resident/patient demographics sync automatically
- Monitoring data flow into existing EHR workflows
- Clinical alerts appear within the EHR — no separate portal required
- Billing documentation generates automatically for PCM time tracking
PCM documentation integrates with the specialist's practice EHR and is shared with the HH agency's system — ensuring all parties have visibility into condition management activities.
Getting Started: Implementing PCM in Your Home Health Agencie
A typical PCM implementation in home health follows a 4–8 week timeline:
- Week 1–2: Specialist practice partnerships, HH agency coordination, patient eligibility criteria for single complex conditions
- Week 3–4: Home management plan templates, caregiver education materials, medication monitoring protocols for home environment
- Week 5–6: Coordination workflows between specialist, CCN Health, HH agency, and caregiver established
- Week 7–8: Patient enrollment starting with post-discharge high-acuity conditions, billing activation, post-HH continuity planning
Home-based PCM succeeds when the specialist is engaged and the caregiver is educated — the management plan must be executable in the home environment by non-clinical caregivers with remote specialist guidance.
Ready to implement PCM in your home health agencie? CCN Health provides full-service Principal Care Management with EHR integration, clinical oversight, and billing optimization purpose-built for home health.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Always consult qualified healthcare, billing, and technology professionals for guidance specific to your facility.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
PCM Program Management
Full Principal Care Management program delivery including enrollment, monitoring, clinical review, and billing documentation — purpose-built for home health workflows.
EHR Integration
Bi-directional integration with Practice EHRs (athenahealth, Epic, Charm Health) ensures monitoring data flows into existing clinical workflows without manual data entry.
Revenue Optimization
~$75–115 per patient per month with PCM. Program stacking with RPM and RTM increases per-patient revenue further.
Specialist at Home
Specialist-level condition management delivered remotely to homebound patients — continuous optimization between appointments.
Post-HH Continuity
PCM continues after home health services end — ongoing specialist revenue and clinical oversight for complex conditions.
Caregiver Partnership
Educated caregivers become active partners in condition management — extending the specialist's reach into the home environment.
Continue Reading
Related Articles
Explore more insights on this topic.
What Is Principal Care Management (PCM)? Eligibility, Billing & Setup
A complete guide to Principal Care Management (PCM) — what it is, who qualifies, how CPT codes 99424/99425 work, and how providers bill Medicare for managing patients with a single high-complexity chronic condition.
Remote Patient Monitoring for Home Health — 2026 Guide
How RPM works in home health — post-discharge vital sign monitoring, hospital readmission prevention, cellular device deployment without facility infrastructure, and Medicare billing for home health agencies.
Chronic Care Management for Home Health — 2026 Guide
How CCM works in home health — bridging episodic skilled visits with continuous care coordination, post-discharge medication reconciliation, and multi-provider communication for homebound patients.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
Principal Care Management (PCM) for home health is a Medicare-reimbursable program. homebound patients with a single dominant complex condition receive specialist-level management between home health visits and specialist appointments, ensuring continuous condition optimization at home. Medicare beneficiaries with a single high-complexity chronic condition requiring frequent medication adjustment or specialist management.
PCM generates ~$75–115 per patient per month through CPT codes 99424, 99425, 99426, 99427. PCM + RPM generates $250–335/patient/month. For rehab patients, PCM + RPM + RTM can reach $350–490/month.
CCN Health integrates with Practice EHRs (athenahealth, Epic, Charm Health) for home health facilities. Home health agencies use practice EHRs rather than facility EHRs. All monitoring data flows bi-directionally between CCN Health and the facility/physician EHR.
Yes — PCM and home health use completely separate billing codes. PCM provides specialist-level condition management while HH provides skilled nursing, therapy, and aide services. They complement each other, with PCM adding the specialist coordination that generalist HH nurses cannot provide.
Yes — PCM can continue indefinitely as long as the complex condition requires specialist management. When the HH episode concludes, PCM transitions from HH-supplemental to standalone specialist coordination. This provides ongoing revenue beyond the episodic care period.
PCM includes caregiver coordination as part of condition management — educating caregivers on symptom monitoring, medication schedules, and when to escalate concerns. Caregivers become informed partners in the management plan rather than passive observers.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.