Clinical
Chronic Care Management for Senior Living — 2026 Guide
How Chronic Care Management works in senior living — care plan development, medication reconciliation, multi-provider coordination, and Medicare billing for residents with multiple chronic conditions.
CCM in senior living provides non-face-to-face care coordination for residents with two or more chronic conditions — including care plan development, medication reconciliation, and coordination across multiple physicians. Unlike RPM, CCM requires no monitoring devices. CCN Health manages the 20+ minutes of monthly clinical staff time required for billing, integrates with ALIS, August Health, and PointClickCare, and generates ~$80–130/patient/month through CPT codes 99490–99491. CCM stacks with RPM for qualifying residents, bringing combined revenue to $255–350/patient/month.
What Is Chronic Care Management (CCM)?
Chronic Care Management (CCM) is a Medicare-reimbursable program that provides non-face-to-face care coordination for Medicare beneficiaries with two or more chronic conditions, including care plan development, medication reconciliation, and coordination across multiple healthcare providers.
Patient eligibility: Medicare beneficiaries with two or more chronic conditions expected to last at least 12 months, placing the patient at significant risk of death, acute exacerbation, or functional decline.
How CCM differs from related programs: CCM requires no monitoring devices — it bills for care coordination time including care plan development, medication reconciliation, and multi-provider coordination. The 2+ chronic condition requirement is the key qualifier.
CCM can be stacked with RPM, BHI for qualifying patients — a single enrolled patient can generate revenue across multiple Medicare programs simultaneously.
Why Senior Living Facilities Need CCM
Senior living residents typically see 3–5 physicians across specialties — a cardiologist, endocrinologist, primary care physician, and others. Without active care coordination, medication conflicts, duplicate tests, and miscommunication between providers are common.
Multi-provider fragmentation: The average senior living resident sees 3–5 physicians who may not communicate with each other — CCM provides the care coordination layer that connects these providers around a unified care plan
Medication complexity: Residents on 8–12 medications are at high risk for drug interactions and adherence failures — monthly medication reconciliation catches conflicts and ensures alignment across prescribers
No device requirement: CCM bills for care coordination time, not device data — making it immediately deployable without hardware logistics, device education, or compliance monitoring
Revenue stacking with RPM: For residents already enrolled in RPM, adding CCM generates an additional $80–130/month per patient with no incremental device cost — only coordination time
How CCM Works in Senior Living — The Clinical Workflow
CCM is a time-based program — billing is driven by documented care coordination time rather than device readings. This makes it operationally simpler than RPM but requires structured care plan management.
Step 1: Eligibility Identification — Identify residents with 2+ chronic conditions (hypertension + diabetes, heart failure + CKD, etc.). Most senior living residents qualify. Obtain patient consent for CCM enrollment and care plan management.
Step 2: Care Plan Development — CCN Health develops a comprehensive care plan documenting all chronic conditions, current medications, treatment goals, and physician contacts. The care plan serves as the coordination roadmap and is shared with all treating physicians.
Step 3: Monthly Coordination — CCN Health clinical staff provide 20+ minutes of monthly care coordination — medication reconciliation, physician communication, care plan updates, transition planning, and patient/family outreach. All time documented for billing.
Step 4: Billing & Documentation — CPT 99490 billed for 20+ minutes of clinical staff time. Complex patients qualifying for physician-level coordination billed under 99491. Additional 20-minute increments captured under 99439.
CCM Does Not Require Monitoring Devices
Unlike RPM, CCM is purely a care coordination program. No monitoring devices, no data transmission requirements, no 16-day compliance thresholds.
- No devices required — CCM bills for care coordination time — care plan development, medication reconciliation, physician communication. No FDA-cleared devices or data transmission needed.
- Optional RPM pairing — When CCM is stacked with RPM, the patient has both device monitoring AND care coordination — but these are billed under separate CPT code families.
The absence of device requirements is CCM's operational advantage — it can be deployed immediately without hardware logistics and scales easily across a large resident population.
CCM Billing: CPT Codes and Revenue
| CPT Code | Service | Reimbursement | Requirement |
|---|---|---|---|
| 99490 | CCM Services | ~$62/mo | 20+ min clinical staff time |
| 99491 | Complex CCM | ~$86/mo | 60+ min physician/QHP time |
| 99439 | Additional 20 min | ~$47/mo | Each additional 20 min |
Estimated monthly revenue per patient: ~$80–130
Program stacking: Stacking CCM with RPM generates $255–350/patient/month. Adding BHI for patients with comorbid behavioral health conditions can reach $303–513/month.
CCM billing requires documented care coordination time — a minimum of 20 minutes per patient per month. Unlike RPM's 16-day device compliance requirement, CCM's threshold is time-based. This makes CCM billing more predictable but requires disciplined time tracking and documentation. In senior living, billing flows through the ordering physician practice.
EHR Integration for CCM in Senior Living
Senior Living facilities typically use ALIS, August Health, PointClickCare for clinical documentation. Most senior living communities use facility EHRs like ALIS or August Health. Physicians use athenahealth, Epic, or Charm Health.
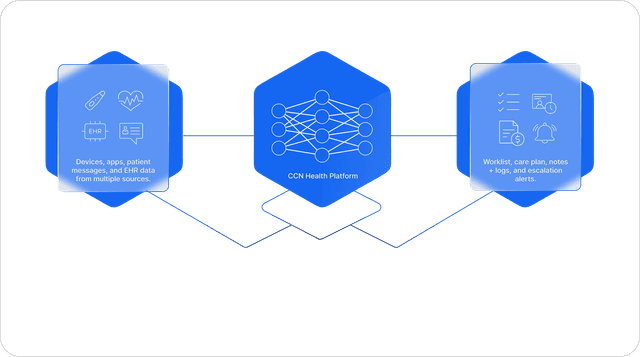
CCN Health provides bi-directional integration with all major senior living EHR systems:
- Resident/patient demographics sync automatically
- Monitoring data flow into existing EHR workflows
- Clinical alerts appear within the EHR — no separate portal required
- Billing documentation generates automatically for CCM time tracking
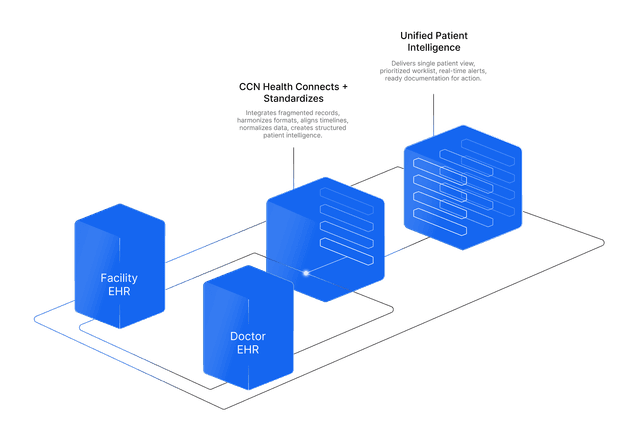
CCM care plans and coordination documentation are shared with the facility EHR (ALIS, August Health, PCC) and the ordering physician's practice EHR. CCN Health ensures all care coordination activities are visible to both the community clinical team and external physicians.
Getting Started: Implementing CCM in Your Senior Living Facilitie
A typical CCM implementation in senior living follows a 4–8 week timeline:
- Week 1–2: Physician practice engagement, resident eligibility screening (2+ chronic conditions), care plan template development
- Week 3–4: Initial care plan creation for enrolled residents, medication reconciliation, physician contact list compilation
- Week 5–6: Monthly care coordination workflows established, time tracking protocols activated, staff orientation on CCM documentation
- Week 7–8: Billing activation, ongoing monthly coordination, care plan revision cycles established (quarterly at minimum)
CCM implementations are faster than RPM because there are no devices to procure, install, or maintain. A community can go from enrollment to billing in 2–3 weeks.
Ready to implement CCM in your senior living facilitie? CCN Health provides full-service Chronic Care Management with EHR integration, clinical oversight, and billing optimization purpose-built for senior living.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or billing advice. CPT code reimbursement amounts are estimates based on CMS published fee schedules and may vary by region, payer, and clinical circumstances. Always consult qualified healthcare, billing, and technology professionals for guidance specific to your facility.
Let's figure this out together
We work closely with every client to find the right approach for their practice. Think of us as your partner, not just a platform.
Topics
Your Partner in Chronic Care
We love working closely with our clients to find the best solutions. Let us help guide you through the complicated stuff.
Why It Matters
Key Benefits
See how this approach drives measurable improvements across your organization.
CCM Program Management
Full Chronic Care Management program delivery including enrollment, monitoring, clinical review, and billing documentation — purpose-built for senior living workflows.
EHR Integration
Bi-directional integration with ALIS, August Health, PointClickCare ensures monitoring data flows into existing clinical workflows without manual data entry.
Revenue Optimization
~$80–130 per patient per month with CCM. Program stacking with RPM and BHI increases per-patient revenue further.
No Devices Needed
CCM is purely care coordination — no hardware procurement, installation, or patient device education required. Deploys in weeks, not months.
Medication Safety
Monthly medication reconciliation catches drug interactions and adherence issues across 8–12 medications prescribed by multiple physicians.
RPM Stack Revenue
Adding CCM to existing RPM patients generates $80–130/month additional revenue with no incremental device cost — pure coordination value.
Continue Reading
Related Articles
Explore more insights on this topic.
What Is Chronic Care Management? Complete Guide to CCM (2026)
A complete guide to Chronic Care Management — what it is, how it works, who qualifies, what services CCM covers, and how providers bill Medicare for care coordination.
Remote Patient Monitoring for Senior Living — 2026 Guide
How Remote Patient Monitoring works in senior living communities — device deployment, wellness-focused monitoring, EHR integration with ALIS and August Health, and Medicare billing for independent and assisted living settings.
Behavioral Health Integration for Senior Living — 2026 Guide
How Behavioral Health Integration works in senior living — PHQ-9/GAD-7 screening for depression and anxiety, addressing social isolation, collaborative care with psychiatric consultants, and Medicare billing.
Common Questions
Frequently Asked Questions
Get answers to the most common questions about this topic.
Chronic Care Management (CCM) for senior living is a Medicare-reimbursable program. residents with two or more chronic conditions receive ongoing care coordination including care plan development, medication reconciliation, and multi-provider communication — all managed remotely without monitoring devices. Medicare beneficiaries with two or more chronic conditions expected to last at least 12 months, placing the patient at significant risk of death, acute exacerbation, or functional decline.
CCM generates ~$80–130 per patient per month through CPT codes 99490, 99491, 99439. Stacking CCM with RPM generates $255–350/patient/month. Adding BHI for patients with comorbid behavioral health conditions can reach $303–513/month.
CCN Health integrates with ALIS, August Health, PointClickCare for senior living facilities. Most senior living communities use facility EHRs like ALIS or August Health. All monitoring data flows bi-directionally between CCN Health and the facility/physician EHR.
RPM monitors vital signs using FDA-cleared devices and bills for device supply and clinical review. CCM coordinates care across providers using care plans and medication reconciliation — no devices needed. They serve different purposes and can be stacked for the same patient, generating combined revenue of $255–350/month.
Most do. CCM requires two or more chronic conditions expected to last 12+ months. The majority of senior living residents have at least hypertension and one additional condition (diabetes, heart failure, COPD, CKD, arthritis). Patient consent is required for enrollment.
Yes — this is called program stacking. RPM monitors vital signs while CCM coordinates care across physicians. They use different CPT code families and can be billed concurrently. Stacking RPM ($175–220/mo) + CCM ($80–130/mo) generates $255–350/patient/month.
Still have questions? We love helping practices figure this out — no pressure, just real answers.
Your Partner in Chronic Care
We're Here to Guide You Every Step of the Way
RPM, CCM, and chronic care management can get complicated. We work closely with every client to figure out the best solutions for their practice.